INTRODUCTION
Mechanical thrombectomy (MT) is an effective, well established and guideline-recommended treatment in patients with acute ischemic stroke (AIS) due to emergent large-vessel occlusion in the anterior circulation [1]. Primary or secondary embolic occlusion of the distal anterior cerebral artery (ACA) affects up to 15% of these patients [2].
The ACA is a branch of the internal carotid artery (ICA) and gives off the anterior communicating artery. Pars precommunicalis is described as A1-segment, pars postcommunicalis as A2-segment. The medial hemisphere is predominantly supplied by the ACA [3]. Circulatory disorders of the ACA typically result to contralateral hemiparesis with accentuation of the lower extremity. Furthermore, a broad spectrum of complex cognitive, behavioral, and emotional disorders are described [4]. Variations of the circle of Willis are well known and described in literature [5-9].
Here we report a case of a patient with an embolic stroke in the area of the ACA due to an occlusion of the proximal A2-segment with the anatomic variation of a triplication, so that occlusion can easily been overseen in computed tomographic (CT)-angiography (CTA). The Institutional Review Board approved the publication of this material.
CASE REPORT
An elderly patient was presented with a severe left sided hemiparesis noticed by nurses of an external hospital while awaking in the morning at 7:00 AM. Last time seen normal was in the night at 10:00 PM the day before emergency hospital admission. The previous hospitalization of the patient was due to an acute decompensated heart failure.
Initial neurological examination documented an altered mental status with severe left sided hemiparesis (greater in leg than arm) with head and gaze deviation to the right in combination with hemineglect to the left, dysarthria and apraxia (National Institutes of Stroke Scale, NIHSS=15 points).
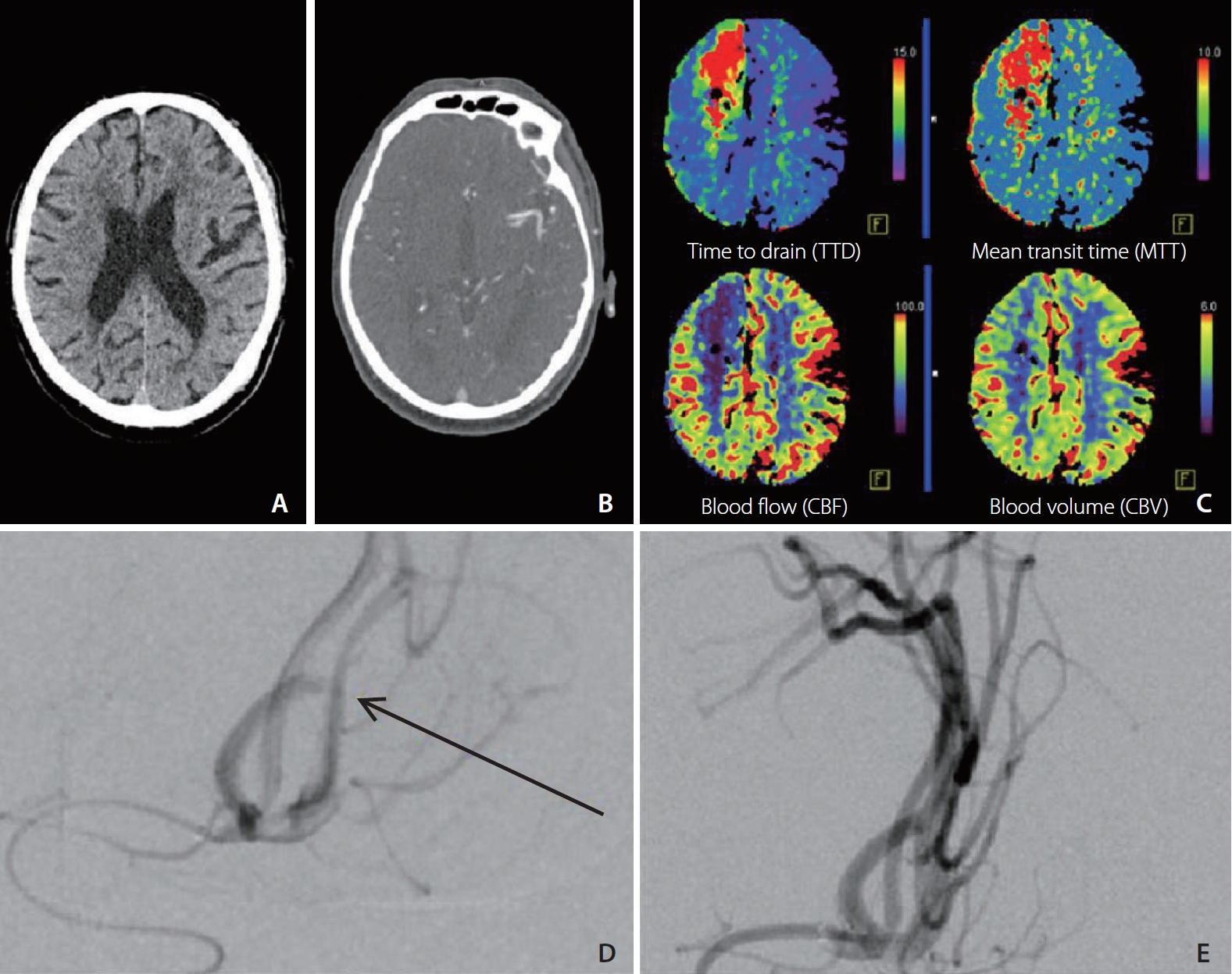
The patient was immediately transferred to our hospital as a “wake-up-stoke”-patient being potentially eligible for recanalization. In this context, the algorithm in our standard operating procedure provides that after exclusion of an intracerebral hemorrhage in the initial non-contrast CT, a CTA and CT-perfusion (CTP) is performed (Siemens Somatom® 64-slice CT system, Syngo® Volume Perfusion CT Neuro software; Forchheim, Germany). Beyond exclusion of an ICH, no early ischemic signs were seen in the non-contrast scan (Fig. 1A). On the first orienting views, no occlusion of intracerebral arteries was detectable (Fig. 1B). However, in CTP the mean transit time in the area of arterial supply of the right ACA was delayed and a congruent cerebral blood flow and cerebral blood volume mismatch was seen (Fig. 1C). As this finding clearly indicates a vessel occlusion, a further much more detailed view on the CTA was performed, where ACA triplication was suspected. Thus, endovascular recanalization was initiated in accordance to German guidelines [10]. Combination with intravenous thrombolysis was not performed, since trials have shown efficacy of intravenous thrombolysis or MT in “wake-up-stroke”-patients [11-13] but still no trial has evaluated a dual recanalization concept in this population.
Interventional angiography revealed occlusion of the proximal A2-segment of the right ACA while confirming a triplication of this segment as an anatomical variation (Fig. 1D). Mechanical thrombectomy resulted in successful recanalization (thrombolysis in cerebral infarction 3, TICI 3) and was performed without complications (Fig. 1E) and no definitive infarct-demarcation in follow-up CT. Due to the continuing unstable cardiac situation, the patient was transferred to our intensive care unit, post-interventionally.
In our advanced diagnostic examinations tachycardiac atrial fibrillation was detected as the underlying cause of the cerebral vascular occlusion.
DISCUSSION
Anatomical variations of the circle of Willis are well described in literature and have an estimated prevalence of 68.2±14.3% [14]. Thus, it should be always been considered that the majority of AIS patients will exhibit one or more anatomic variations. In this context, triplications of the ACA and ACA-branches are described occasionally. Kapoor et al. [6] found triplications of ACA in 2.3% of 1,000 specimen. The clinical significance of the triplication of ACA and ACA-branches is seen minor by some authors [7]. In some cases the triplication is discussed as a risk factor leading to aneurysm [15,16].
In modern diagnostic algorithms of patients with an acute cerebrovascular event, beyond non-enhanced cerebral CT scans, usually also a CTA is included. CTA is especially inevitable in detecting large vessel occlusions. Distal and/or small vessel occlusion can be overseen easily. Moreover, CTP can depict tissue-at-risk in the acute phase and can guide effective acute reperfusion treatment [17,18]. Furthermore CT perfusion maps can improve the detection of vessel occlusions [19]. Nonetheless, the indication for CTP in case of inconspicuous non-contrast and CTA scans is often discussed.
Summarizing, we describe a case of embolic stroke with an occlusion of the proximal A2-segment of a triplicated ACA which was only identified thanks to the additional CTP. The triplication of ACA is a rare anatomical variation, and the occlusion could have been overlooked in case of not performing the CTP sequences. In detecting distal and/or atypical vessel occlusions CTA might be limited in the acute setting, particularly for young residents performing the first view on call. CTP maps improve the diagnostic performance of vessel occlusion detection and should be part of the initial CT-diagnostic algorithm in AIS patients who are basically eligible for recanalization therapies, irrespective of inconspicuous initial findings in CTA.