INTRODUCTION
The Silk stent device is a stent made of woven nitinol stands with low porosity folded in a plastic sheath, characterized by its flexibility and self-expanding properties (with a 2ŌĆō5 mm diameter and 15ŌĆō40 mm length presentation to choose from) [1,2]. Its porosity is 45ŌĆō60%, and it has a 9 mm distal radiopaque tip. It is deployed by careful pressure on the retraction of the delivery line and microcatheter; an advantage of the device is that it can be re-sheathed, even if it has been deployed up to 90%. Also, the conveying system has an improved pusher profile to achieve the best compromise between flexibility and pushability (the ability to transfer force to the distal end from the proximal end of the catheter) [2,3]. Since the introduction of auxiliary stent implantation for the treatment of fusiform aneurysms in the 1990s, in the past decade, Silk stents have been used to maintain blood flow in arteries, excluding aneurysms sacs [1]. These instruments were known as the flow diverter (FD) devices, and they have become critical instruments; several kinds have been used to treat intracranial aneurysms (IAs) over recent years [1,4,5]. The first FD to obtain European Commission approval was the Silk flow diverter (Balt Extrusion, Montmorency, France) in 2008. Eventually, short-and mid-term findings have been reported [1,6,7]. FDs redirect blood flow from the aneurysm, prevent thrombosis development, promote neo-intimal growth along with the mesh, and reconstruct the parent artery [8]. The safety and efficacy of FD treatment for many complex IAs have been recorded in numerous studies [9ŌĆō11]. In the Briganti and collaborators [12] systematic review, more than half of small IAs (56%) were treated with FDs. Despite the vast number of studies on the effectiveness of FDs in treating aneurysms, numerous unexpected adverse effects have also been reported. In addition, there is a lack of research on the problems associated with this approach. Few studies have examined clinical and technological incidents in the use of FDs to treat IAs systematically. The Silk Flow Diverter is a self-expandable stent braided from 48 nitinol wires. The DIVERSION registry is a prospective multicenter study covering all consecutive FD patients in French participating centers between October 2012 and February 2014 [12]. IAs care remains a significant obstacle for modern medicine. In massive subarachnoid dissections and in using multiple clips for artery reconstruction in cases of dysplastic and giant aneurysms, surgical developments have been introduced [13]. However, the Silk FD has shown mounting evidence in the management of this disease; therefore, the primary goal of this study was to determine the effect of the Silk flow diverter device on neurological prognosis and mortality in intracranial aneurysms.
MATERIALS AND METHODS
We followed the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) for the design of this study.
Search
A search for RCT, not-RCT, prospective, and retrospective cohort studies was carried out in SCOPUS (until October 2020), Central Cochrane Registry of Controlled Trials (The Cochrane Library) (until October 2020), MEDLINE (Ovid) until October 2020, EMBASE (Ovid), and PubMed (https://pubmed.ncbi.nlm.nih.gov/) (until October 2020), in addition to the reference list of included studies and other relevant data in potentially eligible studies.
The following search was used: ŌĆ£SILKŌĆØ AND (ŌĆ£flow diverterŌĆØ OR ŌĆ£flow diversionŌĆØ) AND (ŌĆ£MortalityŌĆØ OR ŌĆ£DeathŌĆØ OR ŌĆ£deadŌĆØ) AND (ŌĆ£PrognosisŌĆØ OR ŌĆ£morbidityŌĆØ OR ŌĆ£ComplicationŌĆØ) NOT ŌĆ£AnimalsŌĆØ.
Inclusion Criteria
The studies to be included were screened separately using the following inclusion criteria:
ŌĆó Patients with intracranial aneurysms treated with the Silk device.
ŌĆó RCT, not-RCT, prospective, retrospective cohort studies, case series with more than 20 patients included assessing mortality, functional prognosis type modified Rankin scale (mRS), Glasgow outcome scale (GOS), or another.
Evaluation of the Quality of the Studies Included
The quality of included studies was determined using the NewcastleŌĆōOttawa Quality Assessment Scale; studies with a score of 7 were considered of high methodological quality. Those with scores in the range of 4 to 5 were considered of moderate quality.
Data Extraction, Management, and Statistical Analysis
The following data were extracted: mortality, good functional outcome defined as mRS 0 to 2 points, GOS 4 to 6 points, complete or near-complete occlusion (OŌĆÖKellyŌĆōMarotta CŌĆōD, >90% or another scale) at the end follow-up, rate of retreatment, thromboembolic complications (thrombosis, cerebral infarct, or embolism), and hemorrhagic complications (ruptured aneurysm, subarachnoid hemorrhage, intracerebral hemorrhage). The authors of the included studies were contacted in case of missing data. Doubts were clarified by consensus. Statistical analysis was performed using a pooled rate with the Mantel-Haenszel methodology for each variable. MEDCALC software version 19.2 (MedCalc Software Ltd., Ostend, Belgium) with a randomized effect analysis model was used. Heterogeneity was assessed by calculating chi-square (I2), with high heterogeneity of studies included in the analysis being above 60%.
RESULTS
Search Results
After conducting a systematic search of the information following our strategy, 70 bibliographic citations were identified from PUBMED, SCOPUS, EMBASE, MEDLINE, and Central Cochrane Registry of Controlled Trials (The Cochrane Library). After removing duplicate records, 44 were considered, and among those, 34 were screened. After screening, 20 were excluded, and 14 were potentially eligible based on title or abstract, or both, and full texts were obtained (Fig. 1) [2,6,14ŌĆō25]. All prospective and retrospective observational cohort studies were included.
Overview of Included Studies
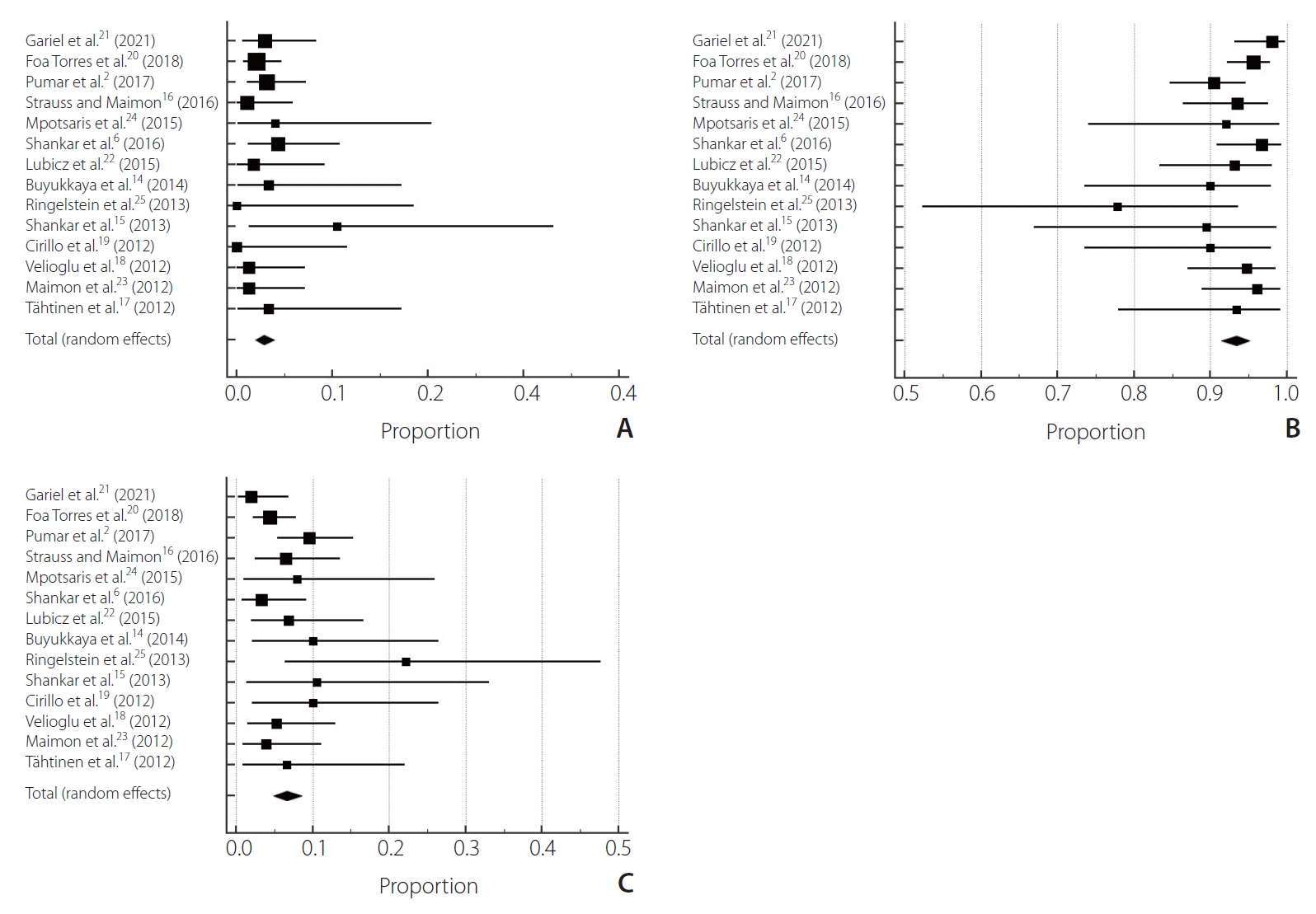
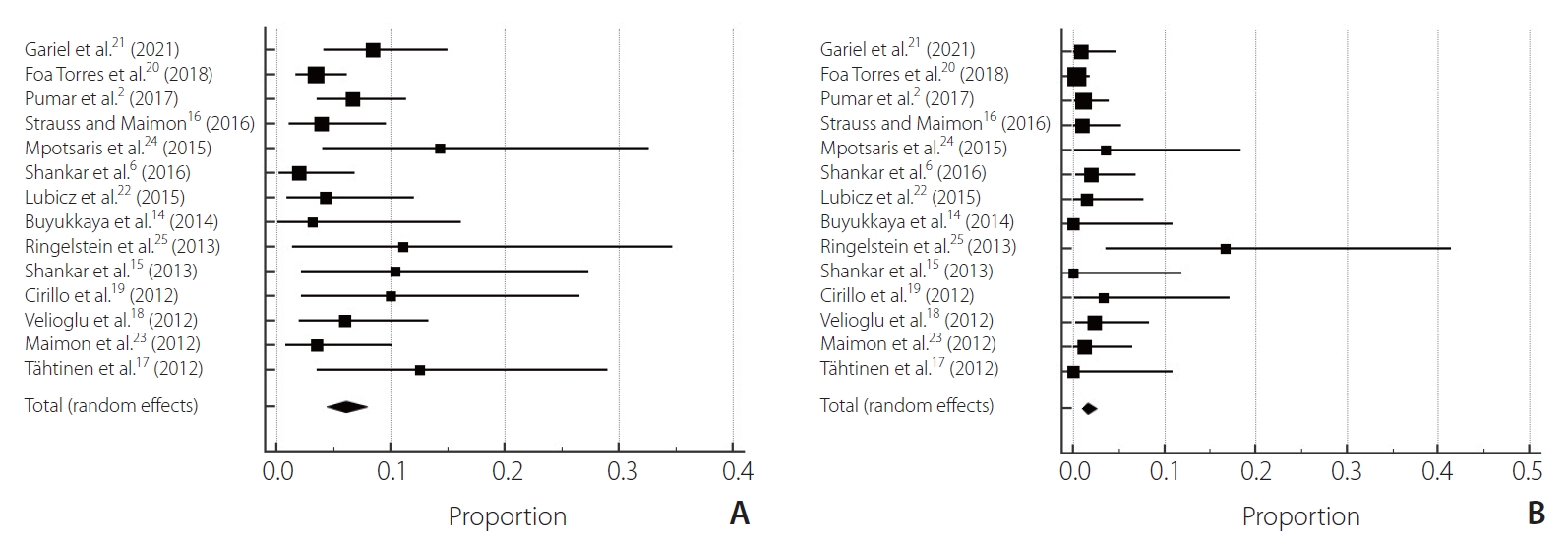
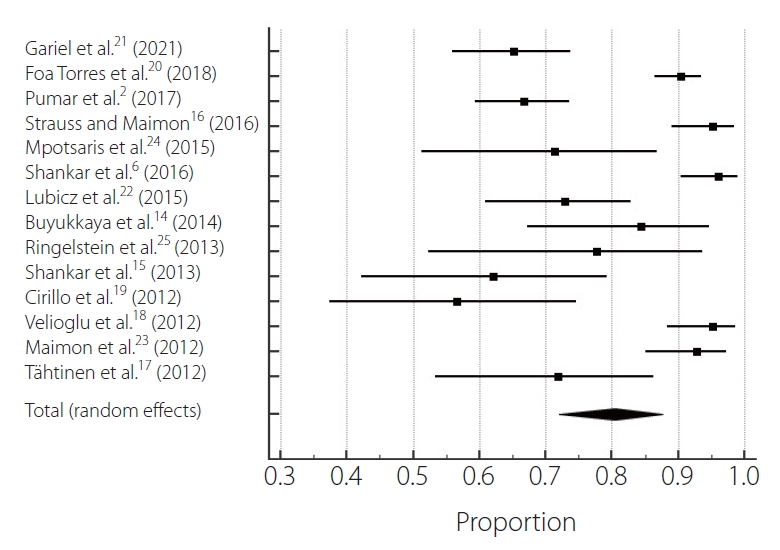
After selection, 14 studies were chosen [2,6,14ŌĆō25], 1 prospective observational cohort study and 13 retrospective observational cohort studies involving 1,021 patients treated for aneurysms [2,6,14ŌĆō20,22ŌĆō25]. The mortality rate was 2.84% (95% confidence interval [CI] 0.00ŌĆō2.75, P=0.83, I2=0%) (Table 1). The clinical good outcomes rate was 93.3% (95% CI 0.00ŌĆō6.23, P=0.15, I2=2.85%). The poor outcome rate was 6.6% (95% CI 0.00ŌĆō6.23, P=0.15, I2=2.85%) (Fig. 2). Regarding complication rates, the total thromboembolic complication rate was 6.06% (95% CI 0.00ŌĆō6.37, P=0.12, I2=3.13%). The total hemorrhagic complication rate was 1.62% (95% CI 0.00ŌĆō5.34, P=0.28, I2=1.56%) (Fig. 3). The complete aneurysm occlusion rate was 80.4% (95% CI 8.65ŌĆō9.38, P<0.0001, I2=9.09%) (Fig. 4).
Risk of Bias
Among the 14 included studies in the analysis, quality assessment was overall good. Three studies scored 7 in NewcastleŌĆōOttawa scale (NOS), 5 scored 6, and 6 scored 5 (Table 2). The funnel plot for all predictors showed different grades of asymmetry (Supplementary Figs. 1ŌĆō3).
DISCUSSION
Combining data from 14 trials, this systematic study and meta-analysis of 1,021 aneurysm patients provide representative data on therapy with the Silk flow diverter to assess clinical outcomes, prognosis, and mortality rates. We have shown that Silk flow diversion treatment is clinically feasible with high technical success rates and high complete occlusion rates and safe with good long-term neurological performance. It should be noted that the complication rates associated with the treatment of these aneurysms have not been negligible.
Our analysis indicated that the mortality rate was 2.84%. In the findings of the studies that were included, some heterogeneity was identified. There is a shortage of research relevant to this methodology on protection and morbidity, so the data added by this study can be helpful. The morbidity and mortality rates were reported in percentage ranges from 2.8 percent to 14.1 percent and 0 percent to 3.7 percent in several recent data studies, respectively, with a permanent morbidity rate of 1.3 percent to 6.3 percent [2,6,14ŌĆō25]. Our research has several merits compared to previously published papers. Since our research covers all the studies available in this important area, it thoroughly reviews all the evidence available in these techniques on adverse events. Due to the rapid growth of the field, we analyzed a larger number of studies. Therefore, we can provide the most definitive summary available at present.
In a prospective Japanese cohort of unruptured IAs, 89.6 percent of the observed 6,679 aneurysms were reported [26]. FDs were used to treat complex and fusiform IAs, rather than small IAs. However, the treatment of small and less complex IAs with FDs has been documented in some studies. Our study showed that the total aneurysm occlusion rate was 80.4 percent (P<0.0001). The aneurysm occlusion rate for the small aneurysm subgroup was 80 percent at 6 months in BrinjikjiŌĆÖs meta-analysis [27]. In a population comprising 1,451 patients with 1,654 treated aneurysms, Brinjikji and colleagues [27] found no impact of aneurysm size on aneurysm occlusion rates. At the 9-month follow-up, Arrese et al. [28] recorded a 76.2 percent aneurysm occlusion rate of 26. No other discrepancies were noticed except for the types of instruments used. In the meta-analysis of Arrese et al. [28], aneurysm occlusions had high heterogeneity in the fixed-effects model. Aneurysm occlusion is a standard criterion that is used to assess intracranial aneurysm therapeutic outcomes. Single-center and multicenter research has shown that the 6-month aneurysm occlusion rate is between 38% and 100% [29]. In those studies with long-term follow-ups, the occlusion rate extension increased with increased time [27ŌĆō29]. According to the meta-analyses by Arrese et al. [28], the occlusion of the aneurysm was 76.2% at a mean follow-up of 9 months.
The treatment of complex intracranial aneurysms with the Silk flow diverter is an effective therapeutic choice. The new Silk stent seems better, despite the delayed complications. In addition, at long-term follow-up, this endovascular approach obtained a high rate of sufficient and stable aneurysm occlusion. The recent implementation of intermediate access catheters also helps to promote endovascular procedures by providing substantial assistance to facilitate and enhance the delivery of stents. The high degree of effective therapy is consistent with previous series [17ŌĆō19,22,30]. A major concern regarding the use of FD stents is the rate of immediate and delayed complications. The good clinical outcome compares favorably with the recent meta-analysis by Murthy et al. [30]. Indeed, in larger intracranial aneurysms in which additional coiling is now recommended, the rate of delayed complications is significantly higher [30]. In previous studies, no recanalization or decrease in occlusion grade was found [22,31].
Our findings demonstrated an overall complication rate of 17%. After Silk flow diverter implantation, there are few reports on acute complications, as most studies report combined rates of acute, subacute, and delayed complications. Most of the complications in our experience were ischemic complications similar to those described by Berge et al. [32]. For Silk flow diverter stents, Berge et al. [32] also reported 7.8 percent transient in-stent stenosis and asymptomatic patients. Like other aneurysm patterning stents, FD stents can induce intracranial hemorrhage and intraluminal stenosis within the parent artery.
The limitations of the present study are a lack of data according to delayed rupture following the endovascular procedure. Our scope did not consider a subgroup analysis according to the follow-up period; also, any resulting differentiation of the Silk flow diverter is a limitation of the present study due to the inability to analyze correspondent data.
CONCLUSION
The Silk diverter device has a good safety and efficacy profile for treating intracranial aneurysms with high complete occlusion rates. With appropriate mortality and morbidity rates in complicated aneurysms, it is a safe care option that is unlikely to be handled with other techniques. There is, however, a chance of neurologic morbidity and ischemic incidents due to the procedure. It is essential to study the mechanism of delayed rupture after flow diversion to determine the required perioperative medication and optimal implantation method. Further studies are needed to provide reliable data on the techniqueŌĆÖs safety and delayed rupture after the procedure.