INTRODUCTION
The Woven EndoBridge (WEB; MicroVention, Aliso Viejo, CA, USA) intrasaccular flow disruptor is a therapeutic option for wide neck bifurcation intracranial aneurysms that does not require the use of adjunctive techniques such as stents or balloon remodelling [1-4]. As with other endovascular devices, displacement of the WEB is a recognized complication. A single case of displacement and subsequent removal of a WEB with an Alligator retrieval device (Medtronic, Dublin, Ireland) has been reported [5]. No reports have been published to date regarding the use of a stent retriever to retrieve a WEB. We describe a case of retrieval of a displaced WEB using a Solitaire Platinum revascularization device (Medtronic, Minneapolis, MN, USA).
CASE REPORT
An unconscious female in her 50s presenting with the World Federation of Neurological Surgeons grade 5 subarachnoid hemorrhage was referred to the Interventional Neuroradiology service for emergent occlusion of a ruptured basilar tip aneurysm.
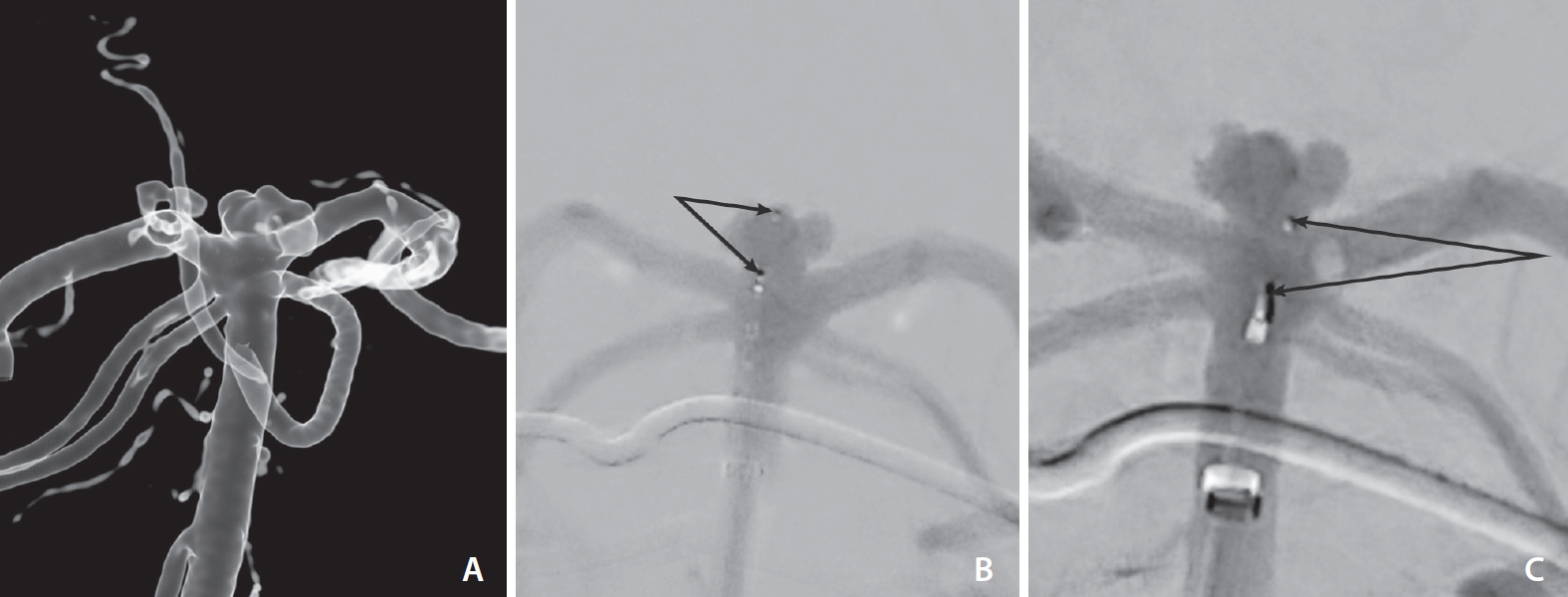
Preliminary angiograms showed a lobulated saccular aneurysm arising from the basilar tip (Fig. 1A). The sac was irregular with a mean diameter of 5 mm and a mean dome height of 3 mm.
The aneurysm was accessed with a VIA 17 microcatheter (MicroVention) through a 6F SOFIA (MicroVention) guide catheter and a 6F Neuron MAX (Penumbra, Alameda, CA, USA) long sheath. A WEB single-layer (SL) 5 mm x 2 mm was successfully deployed into the aneurysm sac (Fig. 1B). However, during detachment, there was a proximal dislocation of the WEB into the distal basilar artery (Fig. 1C).
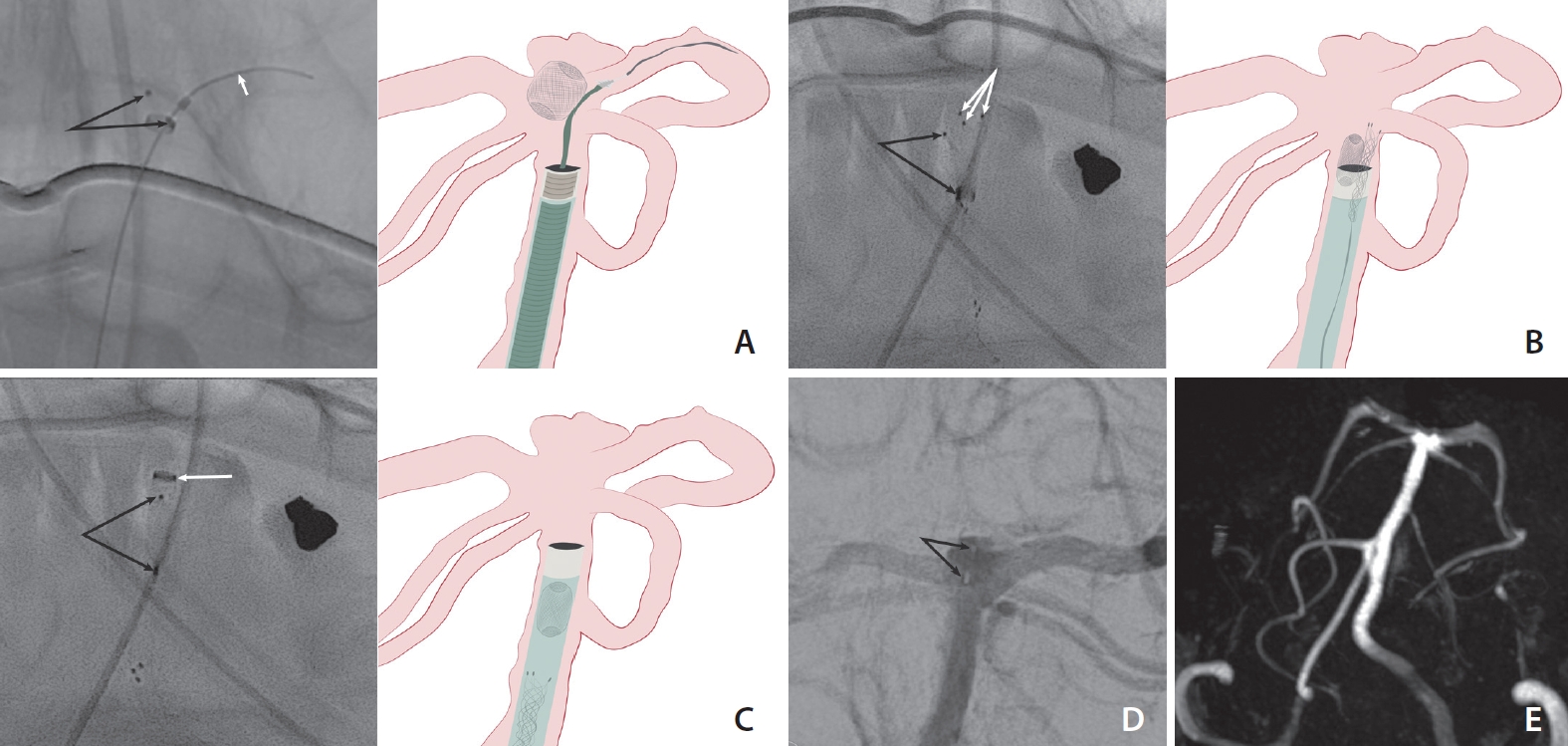
A Headway 21 microcatheter (MicroVention) was navigated over a Synchro microwire (Stryker Neurovascular, Kalamazoo, MI, USA) into the left posterior cerebral artery past the WEB (Fig. 2A). A Solitaire Platinum 4 mm x 20 mm stent retriever was introduced into the Headway. The microcatheter was then pulled back and the Solitaire opened alongside the WEB, partially collapsing it (Fig. 2B). The Solitaire was then pulled back, with the stent retriever providing enough radial force and friction to collapse the WEB and pull it into the SOFIA catheter (Fig. 2C, Supplementary Video 1). The Solitaire, WEB, microcatheter, and guiding catheter were removed as a unit.
Post retrieval angiograms showed no thromboembolic complications or evidence of dissection. The aneurysm was re-accessed with a VIA 17 microcatheter, and a new WEB SL 4.5 mm x 2 mm was then deployed and detached successfully with good wall apposition and satisfactory occlusion (Fig. 2D). The patient was eventually discharged, and follow-up magnetic resonance angiography done at 3 months (Fig. 2E) and 3 years showed complete occlusion of the aneurysm.
DISCUSSION
Displacement of the WEB device is a known complication of its use. In our case, the dislocation likely occurred due to some degree of unrecognized backward tension on the system during the detachment process. Some degree of oversizing of the initial WEB may also have been a factor in displacement; notably, the WEB device that was finally deployed was slightly smaller and this appeared to have been the ideal size, as evidenced by the durable occlusion result on follow-up imaging. Literature on the specific nature and management of this complication has been sparse, with only a single detailed case report on the use of an Alligator device to retrieve the WEB [5].
Stent retrievers or revascularization devices such as the Solitaire Platinum have proven effective in the retrieval of migrated endovascular coils [6,7]. However, there are no known reports of the Solitaire or similar devices having been used to retrieve a displaced WEB.
While the primary reason for the effectiveness of the Solitaire in retrieving the WEB is unknown, we hypothesize that the overlapping design of the Solitaire allowed it to lie along-side the WEB in a constrained space, while providing enough radial force and friction to collapse and pull the WEB into the intermediate catheter. The availability of the left posterior cerebral artery as an initial landing point of the Solitaire also made it possible to achieve a good position relative to the WEB.
A notable point is that the WEB and Solitaire did not remain engaged throughout removal, with the WEB coming to lie within the distal end of the SOFIA catheter. To avoid washing the WEB out and losing it on the way down, the pressurized flush line to the SOFIA was temporarily turned off as the system was carefully pulled out. Some degree of negative pressure, as with a vacuum pressure syringe, may also have been helpful in this case.
CONCLUSION
Deployment and detachment of the WEB device must be performed under strict fluoroscopic control with the utmost care, especially to avoid any degree of forward or backward tension on the system. The Solitaire appears to be a viable option for retrieval of the WEB device, particularly if it can be navigated past the WEB.