INTRODUCTION
Aneurysms arising from the posterior communicating artery (PCoA) account for 25% of total intracranial aneurysms. These comprise a group of aneurysms that include lesions at the junction of the internal carotid artery (ICA) and PCoA, aneurysms of the PCoA itself, aneurysms at the posterior wall of the ICA without incorporating the origin of the PCoA, and lesions of the junction of the PCoA and the posterior cerebral artery (PCA) [1]. A “true” PCoA aneurysm arises from the PCoA itself and is rare—accounting for 0.1–2.8% of all aneurysms [2]. This paper reports a rare case of fusiform aneurysm at the junction of the mid and distal third of the PCoA.
CASE REPORT
A 65-year-old male presented to the casualty with sudden onset, severe headache, and vomiting. The central nervous system examination depicted altered sensorium without motor deficit.
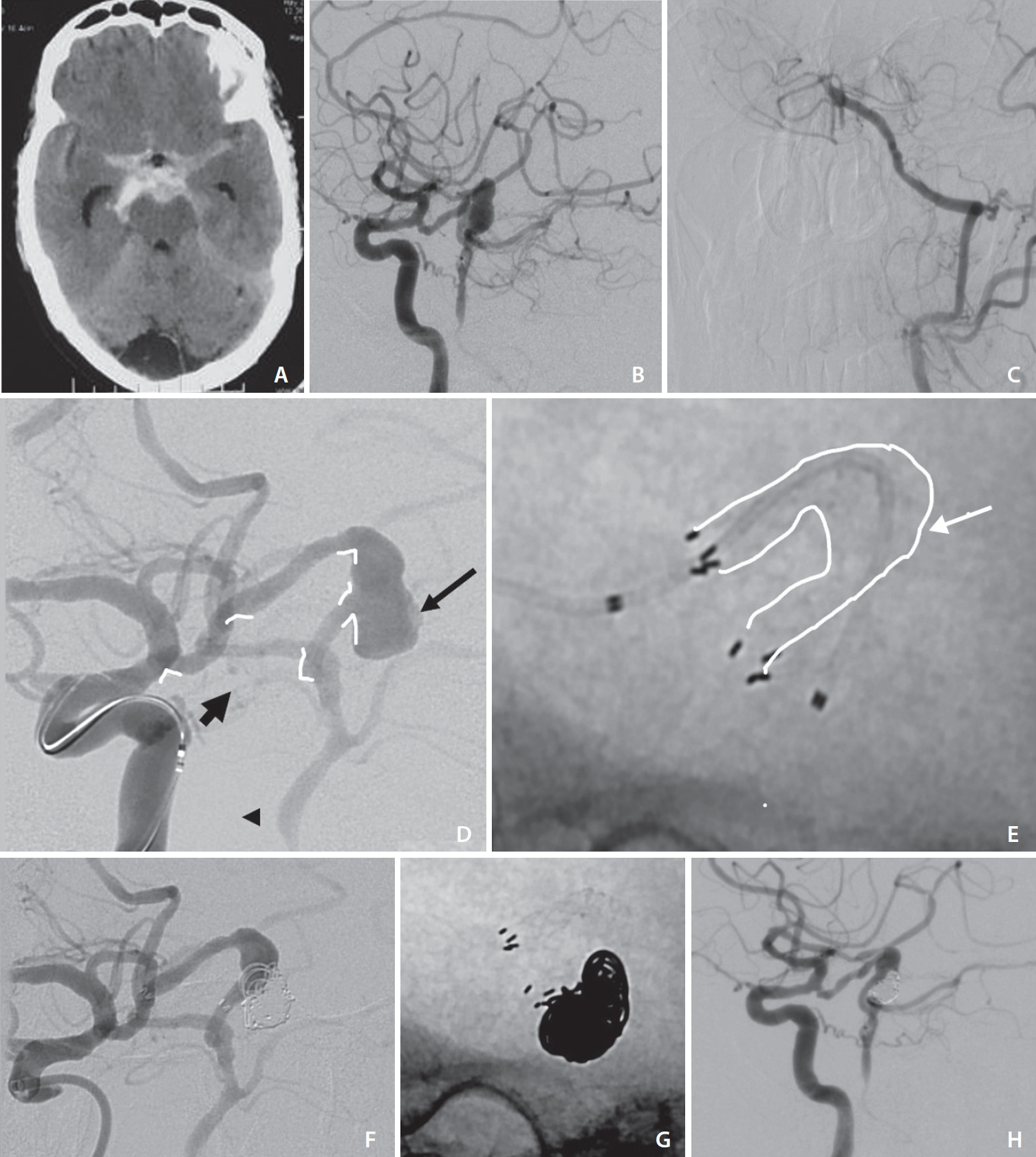
Brain computed tomography (CT) showed diffuse subarachnoid hemorrhage (Hunt and Hess grade 3). Cerebral angiography was performed, which showed occlusion of the proximal third of the basilar artery. There was reformation of the basilar artery through right PCoA. The right PCoA showed a large fusiform aneurysm (approximately 10 mm) in it’s middle third. The distal PCoA had an extremely tortuous course and was at a sharp angle with the right PCA. The left PCoA was mainly supplying the left PCA territory.
Endovascular treatment was planned under general anesthesia. Bilateral femoral puncture was taken. The anatomy of the right ICA, PCoA and the junction of the right PCoA-PCA was extremely tortuous. Multiple treatment options were discussed, and stent-assisted coiling (SAC) was finally planned.
A braided stent (Leo+ baby, Balt) was planned and hence a microcatheter (Vasco+ 17, Balt) was navigated across the aneurysm into the basilar artery. However, when stent deployment was initiated, there was sudden kickback of the catheter and the partially deployed stent fell down into the aneurysm—this was due to extreme tortuosity and different angles between the aneurysm-distal PCoA, PCoA-PCA junction and PCA-basilar artery junction. An attempt was made to deploy an open cell stent as well, however it fell into the aneurysm and had to be removed.
Thus, the plan was changed to oversizing the stent in order to improve distal anchorage—but it would be compatible with Prowler Select Plus microcatheter (Cerenovus), given the size of the PCoA and need for jailing of the second microcatheter. Hence, microcatheter was negotiated across the aneurysm. Enterprise 4.5×30 mm self-expanding stent (Cerenovus) was deployed across the aneurysm to reconstruct the PCoA with jailing of the microcatheter. Enterprise stent, had better anchorage when the kickback of the microcatheter started and could be deployed successfully with jailing of coiling microcatheter. Multiple detachable platinum coils were deployed. The post-operative period was uneventful.
The patient was discharged without any deficit. On clinical follow up at 1 month, the patient was asymptomatic. Follow up CT and CT angiography were performed after 3 months, which showed good patency of stent and no regrowth. In follow-up angiography after 6 months, there was no interval change of the coiled part of the fusiform aneurysm with good reconstruction of the stented segment (Fig. 1).
DISCUSSION
Increased blood flow through the PCoA can induce tortuosity in the vessel, causing increased hemodynamic stress and eventually aneurysm formation. A “true” PCoA aneurysm is an aneurysm that originates from the PCoA itself, rather than from the junction of the ICA and the PCoA [1]. Even among rare true PCoA aneurysms, aneurysms of the proximal PCoA are far more common than in the distal portion.
According to the literature, most cases report a combination of a fetal type PCoA and formation of a true PCoA aneurysm [3]. According to Munarriz et al. [4], hemodynamic stress plays an important role in the treatment of true PCoA aneurysms, as these aneurysms are often associated with a dominant PCoA (fetal type), wherein the PCoA is the major blood supply to the PCA and is associated with a higher flow through it [4]. Hence, preserving the PCoA is of utmost importance, even if it is hypoplastic. The goal in such cases is complete occlusion of the aneurysm while preserving the parent vessel and perforators [5]. In our study, the PCoA is important as it independently supports the posterior circulation by reforming the basilar artery. There was occlusion of the bilateral vertebral arteries in our patient.
Several studies have demonstrated the safety and efficacy of endovascular coiling in true PCoA aneurysms. Yang et al. [6] reported no complications or residual neurological deficits from treating 9 patients endovascularly for a true PCoA. Domingo et al. [5] compared the efficacy of flow diversion and SAC for unruptured non-saccular posterior circulation aneurysms. The results were suggestive of equivalent efficacy regarding occlusion rate, and a lower peri-procedural complication rate with SAC than flow diverter [5]. In a study by Wang et al. [7], successful endovascular therapy (EVT) was achieved in 43 (100%) patients. Of these, 30 patients (69.8%) were treated solely by coiling and did not necessitate remodeling techniques or trapping. This was especially true for narrow necked aneurysms. In cases of wide necked aneurysms, the treatment was slightly more complex. In cases where an acute angle of origin or small caliber of PCoA hindered the implantation of conventional “large profile” stents or balloons, the “the oversize coiling” technique was used despite its higher potential risk of ischemic complications. Only 2 patients had coil migration, while none had ischemic complications [7].
The complex anatomy of true PCoA aneurysms with sharp branch angles within a short distance proves challenging to endovascular access, especially since most of these aneurysms arise within 2–3 mm of the ICA and PCoA junction. The incidence of true PCoA aneurysms is difficult to assess using preoperative angiography because it is challenging to discriminate between this type of aneurysm and junctional aneurysms. Historically, these aneurysms had been treated surgically but technical advances in recent times have made endovascular methods the preferred approach [4]. At times, the acuity of the approach angle may be too sharp to establish a stable microcatheter position. In these cases, balloon-assisted techniques may reduce the risk of possible coil protrusion into the parent vessel [4]. In case of fusiform aneurysms, the use of laser cut stents and stent oversizing may prove helpful.
A major drawback of endovascular embolization is its relatively high recurrence rate. Some studies demonstrate that late retreatment is 6.9 times more likely after EVT [8]. Predictors of angiographic recurrence include aneurysm anatomy, treatment during acute phase of rupture, incomplete initial occlusion, and duration of follow-up [9].
In our case, the challenge was the extremely tortuous anatomy of the ICA, PCoA, and the PCoA/PCA junction. We encountered difficulties in establishing a stable position to deploy the remodeling stent. This could be overcome by an appropriate choice of hardware (stent) and a good distal access catheter placed at the cavernous bend.