Garbled and Incoherent Text Messages Are a Sign of Acute Ischemic Stroke: A New Sign of Aphasia in the Era of Chat Applications
Article information

Abstract
We report a 68-year-old female was diagnosed acute ischemic stroke with an interesting clinical presentation. She was unable to send the messages in chat application normally and accurately. Neurological examination revealed global aphasia without weakness. Computed tomography angiography (CTA) showed the occlusion of the inferior branch of the left M2 of middle cerebral artery (MCA) but showed a good collateral score. Intravenous fibrinolysis and mechanical thrombectomy were not indicated. The patient showed spontaneous clinical improvement and almost fully recovered by the day of hospital discharge. Currently, chat applications have been widely adopted for communication and have replaced direct or telephone conversations in daily life. Dystextia and dystypia may serve as modern sign of aphasia on text conversation.
INTRODUCTION
Acute ischemic stroke is an emergency condition that require early detection and management. Nowsaday, communication is shifting from verbal communication to use social media. We reported a case of aphasic stroke patient who was detected due to garbled and incoherent replies on text messages.
CASE REPORT
A 68-year-old right-handed woman was taken to the hospital because her husband suddenly discovered that she was unable to send messages normally and accurately via a chat application. He detected a trivial problem at noon. Her increasingly awkward responses became more evident in the evening when she sent mostly pictures, known as stickers, in the chat application. By then, some of her answers were utterly inappropriate for the questions. She texted her husband’s questions instead of answering them. However, some of her responses were understandable from a spoken language standpoint (Fig. 1). Her husband immediately visited the patient and found out she was not speaking or following his commands.
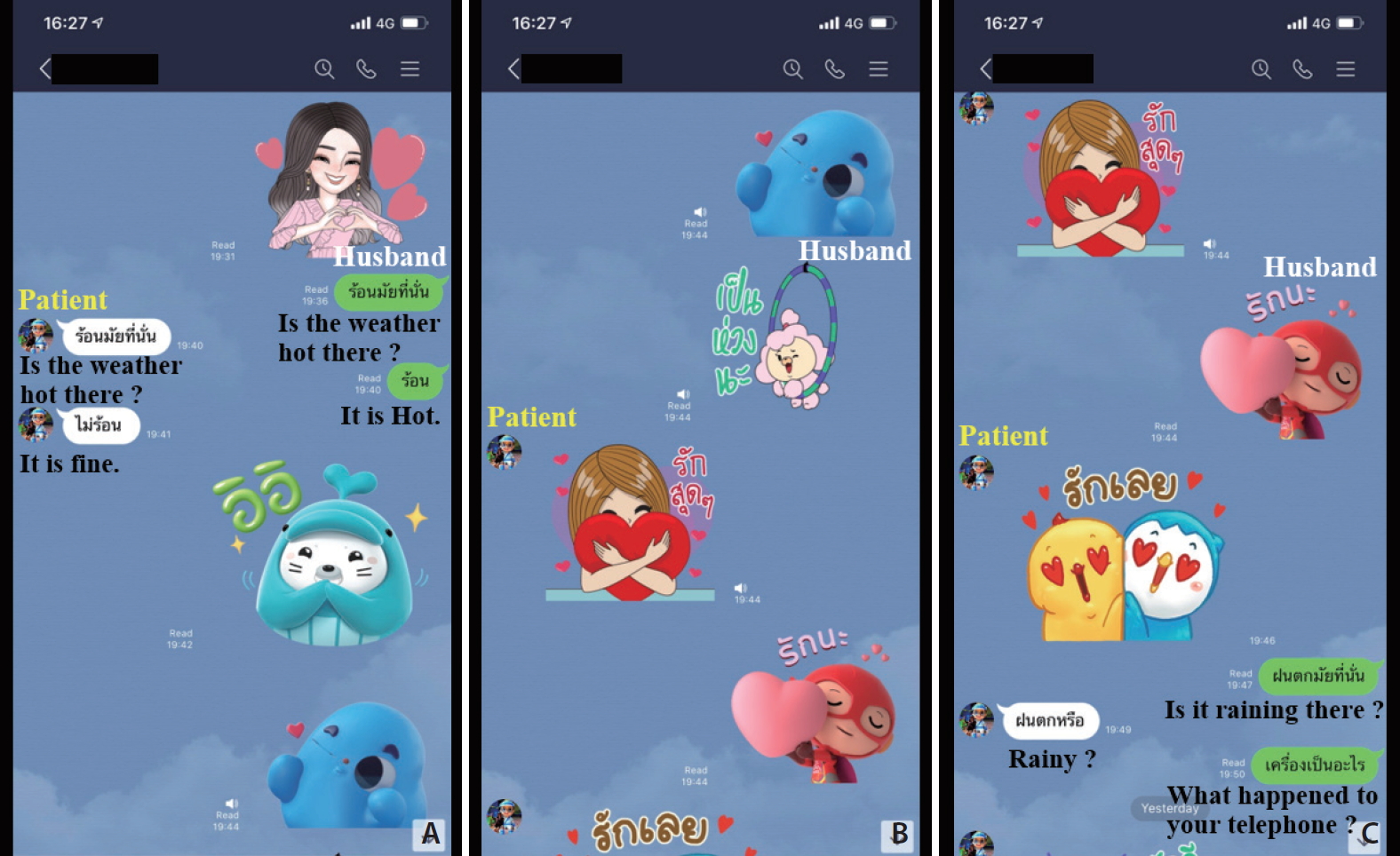
Conversation in the chat application revealed garbled and incoherent answers. (A) The husband asked, “Is the weather hot there?” The patient repeated after him, “Is the weather hot there?”. (B) The patient sent many pictures (stickers) to her husband instead of text conversation as she usual does. (C) Her husband asked, “Is it raining there?” The patient answered, “rainy?”.
On arrival at our hospital, she had global aphasia. She was alert but had fluent speech impairment, along with impaired comprehension, repetition, and naming. The examination of the cranial nerves was unremarkable. Muscle strength showed normal motor function in all extremities. The patient had a National Institutes of Health Stroke Scale (NIHSS) score of 6. She then underwent computed tomography (CT) of the brain, which demonstrated acute infarction at the posterior part of the left temporal, insular, and parietal lobes. There was an incidental finding of meningioma at the right anterior temporal pole convexity (Fig. 2). An occlusion of the inferior branch of the left M2 of MCA was found via multiphase CT angiography (CTA) but showed a good collateral score. Intravenous fibrinolysis and mechanical thrombectomy were not performed because the clinical symptoms rapidly improved with mildly-impaired speech and comprehension. Besides, there was no large vessel occlusion in the CTA brain. The electrocardiogram (ECG) revealed atrial fibrillation rates of 80 to 90 beats/min. Echocardiography demonstrated good ejection fraction (60%). Neither intracardiac thrombus nor valvular heart disease was detected.

(A) and (B), Non-contrast computed tomography (NCCT) brain scan performed 9 hours after the onset of stroke demonstrated early acute infarction at the posterior part of the left temporal, insular, and parietal lobe (white arrows). (C) Hyperdense MCA sign (arrowhead) at the inferior branch of the left M2 of MCA. (D) The incidental finding of meningioma at the right anterior temporal pole convexity (black arrow).
The provisional cause of stroke was cardioembolism. Acute infarction areas were clearly seen in the pre-existing areas in a follow-up CT brain scan at 72 hours, but no hemorrhagic transformation was observed (Fig. 3). Standard stroke care was provided, and an oral anticoagulant was initiated for secondary stroke prevention. The patient showed spontaneous clinical improvement, and she had almost fully recovered by the day of hospital discharge. After the recovery, she explained that she wanted to send the text message, but she lost language comprehension and could not type the messages at that time.
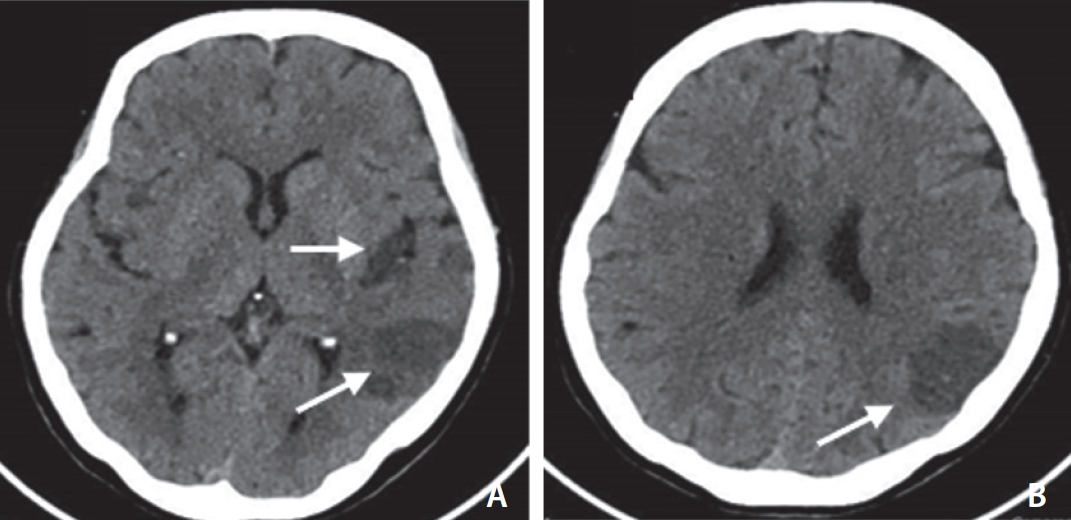
(A) and (B), Non-contrast computed tomography (NCCT) brain done after 72 hours, obviously seen acute infarction at the posterior part of the left temporal, insular, and parietal lobe (white arrows).
DISCUSSION
Aphasia is a loss or impairment of verbal communication, writing, and reading difficulties [1]; 80–90% of aphasia is caused by stroke [2]. The patients suffer from an inability to communicate with others. In the past decade, mostly aphasic stroke patients were detected by witnesses. With the current COVID-19 pandemic, social distancing has been encouraged in daily life. Communication has shifted to using social media, and chat applications have been widely adopted for communication and have often replaced direct face to face or telephone conversations.
The new terms ‘dystextia’ and ‘dystypia’ have been established. These new terms refer to impairment in texting and typing. A case series and literature review by Sharma AK et al on dystextia and dystypia in stroke patients found that aphasia occurs in 86% of cases. A typical lesion is in the left posterior insula, although a brain lesion specific for dystextia and dystypia remains unclear [3]. Garbled replies in texts should elicit and draw public attention of a stroke sign in modern society.
It is currently well known that social media has demonstrated benefits in many aspects of stroke medicine, whether it be knowledge dissemination to the patients, medical education, or medical research [4]. The mnemonic “FAST” is crucial for public concern of stroke. The mnemonic “FAST” is useful for identifying stroke signs that refer to Face drooping, Arm weakness, Speech, and Time to call 9-1-1, where it was found that it could identify 88% of carotid artery distribution strokes [5,6]. In this era, errors in texts in chat applications should be considered as a stroke sign. This may provide a benefit for early stroke detection in patients whose language problems indicate a symptom onset of stroke.
Notes
Fund
None.
Ethics Statement
The patients/participants provided written informed consent for the publication of this case report. IRB approval number: COA. MURA2020/961.
Conflicts of Interest
The authors have no conflicts to disclose.
Author Contributions
Concept and design: CK, BS, and AB. Analysis and interpretation: CK. Data collection: CK and BS. Writing the article: CK, BS, and AB. Final approval of the article: CK, BS, and AB.