INTRODUCTION
This report illustrates the endovascular management of a growing brain aneurysm in a child with PHACE syndrome (OMIM 606519), a rare non-inherited congenital neurocutaneous syndrome with unknown etiopathogenesis wherein cerebrovascular malformations are the most common extra-cutaneous abnormalities [1-3]. Endovascular management of brain aneurysms in young children can be challenging due to small parent vessel diameters, non-availability of specialized low profile microcatheters, and relative contraindications to stent or flow diverter placement due to the changes that are anticipated with the childŌĆÖs growth [4,5]. These challenges are further exacerbated when intracranial aneurysms occur in the setting of syndromic cerebrovascular abnormalities such as PHACE. It is hoped that perusal of this report will (1) enhance the familiarity of readers with PHACE syndrome, (2) highlight the adaptation of the novel low-profile SMB to perform balloon assisted coiling (BAC) in a child, and (3) demonstrate the feasibility of utilizing the persistent trigeminal artery (PTA) to gain internal carotid artery aneurysm sac access from a posterior circulation approach.
CASE REPORT
The patient had initially presented to our center as an infant for the management of multiple cerebrovascular abnormalities that had been discovered on a computed tomography angiogram, and digital subtraction angiogram (DSA) of the head that had been performed at an outside center as part of the work up for PHACE syndrome. That work up had been initiated by the presence of a progressing facial hemangioma, left eye ptosis, and a cardiac murmur. These initial imaging studies had revealed persistent fetal circulatory patterns in the form of an aberrant left internal carotid artery (which also gave rise to a prominent ascending pharyngeal branch) with a narrow cervical segment and postero-lateral course at the skull base, and a prominent PTA between the cavernous segment of the left internal carotid artery (LICA) and the mid-basilar artery. In addition, the more superior segments of the LICA were dysplastic with segmental narrowing and dilatation, and the entire right ICA, (which terminated at the communicating segment) was also extremely dysplastic with a tortuous corkscrew course. The upper basilar artery was significantly narrowed with multiple moyamoya like perforating arteries arising from the top of the basilar artery as well as the terminal regions of the internal carotid arteries. The right anterior cerebral artery and middle cerebral artery were exclusively supplied from the LICA via the Anterior communicating artery.
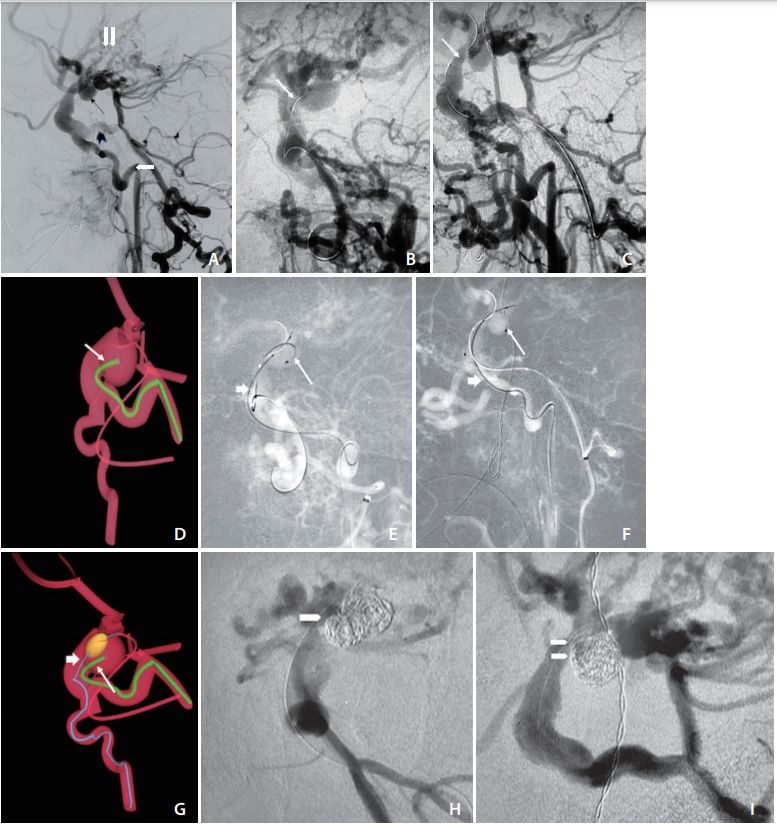
Bilateral posterior communicating artery (PCoA) segment aneurysms were noted, as well as a top of basilar aneurysm and very dysplastic aneurysmal regions at the junction of the right PCoA and the right posterior cerebral artery (Fig. 1A). These malformations were observed with serial magnetic resonance angiographic (MRA) imaging, performed at 6, 12, and 24 months following the initial imaging studies. A significant enlargement of the left posterior communicating artery aneurysm (PCOM) aneurysm from 4├Ś5├Ś4 mm to 7├Ś5├Ś8 mm was reported on cross sectional MRA between the second and third follow up studies mentioned above. We then decided to opt for endovascular treatment of this growing left PCoA aneurysm. This decision was based upon the increased risk of rupture posed by this growing aneurysm, the relatively higher operative risk associated with surgical clipping in the setting of multiple vascular malformations and variations, and our experience with endovascular management of cerebrovascular pathology in the patientŌĆÖs age group. In terms of endovascular treatment paradigms, although flow diversion was considered, the narrowing of the proximal ICA, as well as the anticipated need for future surgical bypass procedures (for moyamoya like changes) resulted in not proceeding with this option [6-8]. Likewise, it was thought best to avoid stent placement within the intracranial arteries.
Treatment
Bilateral common femoral arterial access was obtained under ultrasound guidance. Anticoagulation was obtained with the intrvaneous administration of 100 units of Heparin per kilogram body weight. We then selected the left common carotid artery using a 4 French, 65 cm angle glide catheter advanced through a 4 French arterial sheath placed in the left common femoral artery. The left vertebral artery was selected via a right groin access with a 5 French, 115 cm Sofia intermediate catheter (Microvention, Aliso Viejo, CA, USA). Simultaneous contrast injections were performed through both catheters, initially for diagnostic DSA; and thereafter to obtain digital road maps that delineated the LICA, the left vertebral artery and basilar artery clearly. The left PCoA aneurysm was noted to be 11.2├Ś7├Ś6 mm in size, it had a complex shape and a wide neck (6 mm). We then advanced an Echelon 10 (Medtronic, Irvine, CA, USA) over a Synchro soft microwire (Stryker Neurovascular, Fremont, CA, USA) through the Sofia catheter into the basilar artery and the PTA was selected. The Echelon 10 microcatheter was then very carefully advanced across the PTA to safely catheterize the LICA (Fig. 1BŌĆōD). Subsequently, we prepared a Scepter-mini balloon microcatheter (Microvention) over an Asahi 0.008 inch microwire (Medtronic) without ex-vivo pre-inflation as described elsewhere [9]. The balloon microcatheter was then advanced through the angle glide catheter into the narrow segment of the proximal LICA and eventually into the intracranial ICA such that the balloon markers were across the neck of the PCOM aneurysm (Fig. 1EŌĆōG). The diameter of the LICA at this site was 1.9 mm, and the Scepter mini balloon has a nominal diameter of 2.5 mm, and length of 9 mm. Subsequently, Multiple hydrogel coated platinum coils were then placed into the aneurysm sac through the Echelon 10 microcatheter, while the aneurysm neck was remodelled with inflation of the Scepter mini balloon, and complete obliteration of the aneurysm was achieved (Fig. 1H, I). A total of 35 mL of Iodinated Contrast was used for the procedure.
DISCUSSION
Our report illustrates some of the common cerebrovascular malformations found in children with PHACE syndrome as well as a trans PTA approach for performing balloon assisted aneurysm coiling in a child with this syndrome. PHACE syndrome has a low prevalence in the general population (<1:1,000,000). However, it is not infrequent for cerebrovascular specialists working in large pediatric centers to encounter children affected by this disorder. Such children, who often present for evaluation of cutaneous malformations are eventually diagnosed with PHACE syndrome on further workup by a multidisciplinary pediatric vascular clinic. The cerebrovascular malformations that can be found in these children are those illustrated here, such as persistent primitive embryonic arteries, agenesis or stenosis of the internal carotid and vertebral arteries, moyamoya disease like intracranial arterial changes; and fusiform and saccular intracranial aneurysms [1,10].
The SMB was considered to be the best choice for BAC in this child due to its low profile (which enabled us to advance it through a narrowed segment of the ICA in an atraumatic fashion, while using just a 4 French angled glide diagnostic catheter for support), as opposed to other balloon microcatheters, such as Scepter C or XC; Hyperform/Hyperglide (Medtronic), Transform (Stryker Neurovascular) etc., that could also have been used, but have larger inflation profiles. The SMB also has a maximum inflation diameter of 2.7 mm, that mitigates against inadvertent balloon overinflation within the small caliber intracranial arteries found in children. Similarly, the Echelon 10 microcatheter (Medtronic) was utilized due to its low profile as well as its unique torqueability which allowed for the catheterization of the aneurysm at a difficult backwards angle.