The Woven EndoBridge Device for the Treatment of Intracranial Aneurysms: Initial Clinical Experience within an Australian Population
Article information
 , Julian Maingard, BBiomedSci, MBBS, FRANZCR, EBIR2,3,4, Michelle Foo, MBBS2, Yifan Ren, MD2, Anthony Lamanna, MD2, Daniel Nour, MBBS5, Jonathan Hall, MBBS, FRANZCR5, Dylan Kurda, MD, FRANZCR, EBIR6, David Tan, MBBS7, Shivendra Lalloo, MBChB, MSc, FC Rad, FRANZCR, EBIR6, Ramon Martin Francisco Bañez, MD, FRANZCR3, Jeremy Russell, BSc/BE (Hons), MBBS (Hons), FRACS8, Lee-Anne Slater, MBBS (Hons), MMed, FRANZCR, CCINR3, Ronil Vikesh Chandra, MBBS, MMed, FRANZCR, CCINR3, Winston Chong, MBBS, FRANZCR, CCINR3, Ashu Jhamb, MBBS (Hons), FRANZCR, CCINR, EBIR5, Duncan Mark Brooks, MBBS, FRANZCR, CCINR, EBIR2, Hamed Asadi, MD, PhD, FRANZCR, CCINR, EBIR, FCIRSE, EBNI2,3,6,7,8
, Julian Maingard, BBiomedSci, MBBS, FRANZCR, EBIR2,3,4, Michelle Foo, MBBS2, Yifan Ren, MD2, Anthony Lamanna, MD2, Daniel Nour, MBBS5, Jonathan Hall, MBBS, FRANZCR5, Dylan Kurda, MD, FRANZCR, EBIR6, David Tan, MBBS7, Shivendra Lalloo, MBChB, MSc, FC Rad, FRANZCR, EBIR6, Ramon Martin Francisco Bañez, MD, FRANZCR3, Jeremy Russell, BSc/BE (Hons), MBBS (Hons), FRACS8, Lee-Anne Slater, MBBS (Hons), MMed, FRANZCR, CCINR3, Ronil Vikesh Chandra, MBBS, MMed, FRANZCR, CCINR3, Winston Chong, MBBS, FRANZCR, CCINR3, Ashu Jhamb, MBBS (Hons), FRANZCR, CCINR, EBIR5, Duncan Mark Brooks, MBBS, FRANZCR, CCINR, EBIR2, Hamed Asadi, MD, PhD, FRANZCR, CCINR, EBIR, FCIRSE, EBNI2,3,6,7,8
Abstract
Purpose
Advances in endovascular technology have expanded the treatment options for intracranial aneurysms. Intrasaccular flow diversion is a relatively new technique that aims to disrupt blood inflow at the neck of the aneurysm, hence promoting intrasaccular thrombosis. The Woven EndoBridge device (WEB; MicroVention, Aliso Viejo, CA, USA) is an US Food and Drug Administration approved intrasaccular flow diverter for wide-necked aneurysms. We report the early interim clinical and radiological outcomes of patients with both ruptured and unruptured intracranial aneurysms (IAs) treated using the WEB device in an Australian population.
Materials and Methods
A retrospective analysis was done of patients with ruptured or unruptured IAs who received treatment with WEB across 5 Australian neuroendovascular referral centers between May 2017 and November 2020. Angiographic occlusion was assessed with time-of-flight magnetic resonance angiography. Complications were recorded and clinical outcomes were assessed using the modified Rankin scale at follow-up.
Results
In total, 66 aneurysms were treated in 63 patients, with successful deployment of the WEB device in 98.5% (n=65). Eighteen (26.9%) ruptured aneurysms were included. Failure of deployment occurred in a single case. Adjunct coiling and/or stenting was performed in 20.9% (n=14) cases. Sixty-two patients with 65 aneurysms using a WEB device were followed up (mean=9.1 months), and 89.4% of these had complete aneurysm occlusion while 1.5% remained patent. Functional independence was achieved in 93.5% of cases.
Conclusion
Early results following the use of WEB devices in Australia demonstrate safety and adequate aneurysm occlusion comparable to international literature.
INTRODUCTION
Intrasaccular flow diversion has an established role in the management of intracranial aneurysms. Ruptured intracranial aneurysms (IAs) are the most common cause of spontaneous subarachnoid hemorrhage (SAH). The prevalence of unruptured IAs varies from 3–5% [1]; and whilst rupture risk is related to aneurysm size and location with the majority remaining unruptured, in cases of rupture causing SAH, patients are at high risk of significant morbidity with a mortality rate of up to 50% [2]. After the International Subarachnoid Hemorrhage Trial (ISAT) demonstrated higher disability-free survival rates in patients who received endovascular treatment compared to neurosurgical clipping, both ruptured and unruptured aneurysm treatment continues to shift towards endovascular coiling [3]. Since ISAT, advances in endovascular technology and techniques have expanded the armamentarium available to the neurointerventionist. Balloon-assisted and stent-assisted approaches permit treatment of complex aneurysms previously deemed untreatable using endovascular techniques, such as those with difficult morphology or in difficult locations. More recently, flow diverting stents and various scaffolding devices allow the treatment of giant and wide-necked aneurysms with greater effectiveness [4]. Intrasaccular flow diversion is a more novel technique that disrupts inflow at the neck of the aneurysm, promoting subsequent intrasaccular thrombosis. The Woven EndoBridge device (WEB; MicroVention, Aliso Viejo, CA, USA) is a US Food and Drug Administration approved intrasaccular flow diverter for wide-necked aneurysms. Early meta-analysis data demonstrated a good safety profile, with intermediate-term complete and adequate occlusion rates of 39% (26–52%) and 85% (78–91%) respectively [5]. Following this, the multicenter, prospective, single-arm WEB-IT trial reported a technical success rate of 98.7%, with only 1 primary safety event (0.7%) and adequate occlusion in 84.6% of patients at 12 months [6,7].
Data from 3 Good Clinical Practice studies including WEBCAST, FRENCH Observatory, and WEBCAST-2 with a pooled cohort of 168 patients with 169 wide-necked aneurysms (≥4 mm) demonstrated complete occlusion in 52.9% and adequate occlusion in 79.1% after 1 year. A neck remnant was seen in 26.1% of participants and an aneurysm remnant in 20.9%. Retreatment was performed in 6.9% of cases [8]. These results compared favorably to pooled results for endovascular coiling of wide-necked aneurysms in 2,446 patients, with 2,556 aneurysms from 38 studies with a near-complete occlusion rate of 74.5% with retreatment rates of 5.8% [9].
In Australia, there has been limited implementation of WEB treatment limited to a few Neurointervention centers, leading to substantial institutional and practitioner variation in the management of candidate intracranial aneurysms as well as the follow-up and surveillance of aneurysms treated with WEB. Whether this influences patient outcomes is unknown, although it represents a major knowledge gap in practice. This multicenter study is the first to report the initial clinical experience and early interim results of the WEB device when used to treat ruptured and unruptured aneurysms in a large series within an Australian population.
MATERIALS AND METHODS
Population
A retrospective analysis was performed across 5 Australian tertiary neuroendovascular referral centers, with inclusion of patients with ruptured and unruptured intracranial aneurysms treated with the WEB device between May 2017 and November 2020. This study was approved by the institutional human research ethics committee. As specific patient information such as age or sex is not included, informed consent for publication was not required. All procedures were performed by experienced neurointerventionists (JM, DK, SL, RMFB, LS, RC, WC, AJ, DMB, and HA) and treatment decisions were made by a multidisciplinary team consisting of neurointerventionists and neurosurgeons after discussion with the patient.
Wide-necked aneurysms (i.e., neck width >4 mm and/or dome-to-neck ratio >2) were considered for treatment if the overall aneurysm morphology and location (i.e., lesion axis relative to parent vessel) appeared amenable to WEB deployment. Aneurysm sizes with a neck width of 3–10 mm and height between 3–10.5 mm were eligible to be treated with WEB and were able to accommodate the available device sizes smallest: WEB 17 single-layer (SL, 3×2 mm diameter) to largest: WEB 11 single-layer sphere (SLS, 11×9.6 mm diameter). With regards to aneurysm shape, the WEB systems are spherical (SLS) or cylindrical (SL) in shape, therefore unilobular aneurysms with spherical, cylindrical, or ovoid-shaped morphology are ideal for WEB deployment. The treatment approach was at the discretion of the treating neurointerventionist, depending on individual anatomical considerations, and aneurysms with unfavorable morphology or dimensions outside the available device sizes were excluded.
Device
The WEB device is a braided nitinol wire structure of various shapes and sizes. Both SL and SLS designs are available, ranging from SL 4×3 mm smallest to 11×9 mm largest; SLS diameter 4 to 11 mm, height 2.6 to 9.6 mm. Proximal and distal platinum markers assist in visualization during deployment. The WEB device has increased metal coverage at its base (almost 100% at its center) [10] resulting in a smooth mesh surface that diverts flow from the parent vessel away from the aneurysmal sac. Postoperatively, if no WEB protrusion is evident and no other stenting was performed, the patient may be treated with a single antiplatelet agent (aspirin) for 5 to 6 weeks, thus potentially avoiding the need for prolonged dual antiplatelet therapy [11]. These features make the WEB device a suitable treatment option for both ruptured and unruptured aneurysms [12].
All procedures were performed as per conventional aneurysm coil treatment under general anesthesia, procedural intravenous heparin, and with varying dual antiplatelet loading regimens in elective cases. Continuous heparinized saline flush with or without nimodipine was used during the procedure. Triaxial access was obtained using a long guidesheath in the proximal internal carotid, subclavian, or vertebral artery, a distal access catheter in the intracranial internal carotid artery (ICA) or vertebral artery, and a microcatheter within the aneurysm. The device is deployable from a microcatheter with inner diameters ranging from 0.021 to 0.033-inch, depending on the size and shape of the device, which was selected at the discretion of the treating neurointerventionist. The WEB device was sized based on width and dome height measurements obtained during 3D digital subtraction angiography using a continuous column of contrast via an injecting pump. The device was generally oversized by approximately 1 mm to ensure close apposition of the device along the aneurysm wall. During deployment, the WEB device opens up such that the base of the device is retracted to lie across the neck of the aneurysm. Control angiography is performed to confirm appropriate placement and to check for platelet aggregation prior to release of the device. Final angiography confirms aneurysm occlusion.
Anatomical Outcome
Immediate angiographic occlusion was graded at the time of the procedure by the treating neurointerventionist as per the WEB occlusion scale (WOS) [10] or modified Raymond–Roy occlusion classification (mRROC) [13]. The WOS is an angiographic assessment scale for reporting aneurysm occlusion achieved with intrasaccular mesh implants. WOS A&B indicate complete occlusion without an angiographically visible collection of contrast within the marker recess. Residual neck (WOS C) is defined as the presence of contrast in contact with the aneurysmal neck that does not contact the wall of the aneurysmal sac or the inside of the WEB device, while a residual aneurysm (WOS D) is defined as apparent contrast in contact with the aneurysmal sac or inside the WEB device. The mRROC was employed when evaluating coiled aneurysms and is defined as class I (complete obliteration), class II (residual neck), class IIIa (residual aneurysm with contrast within coil interstices), or class IIIb (residual aneurysm with contrast along aneurysm wall). All patients had early (within 1 week of deployment) and mid-term follow up (mean 9.1 months) with magnetic resonance imaging (MRI) including magnetic resonance angiography (MRA) with 3D time-of-flight (TOF) technique, which were independently reviewed using multiplanar reformats by experienced neurointerventionists, who were blinded to treatment approaches and outcomes.
Clinical Outcome
Clinical outcome was assessed using the modified Rankin scale (mRS) at follow-up within 6 weeks following treatment. Complications were recorded in the procedural report and were readily available for review.
RESULTS
A total of 67 aneurysms in 64 patients were identified with attempted WEB treatment with an overall successful deployment of the WEB device in 98.5% (n=66) of cases. Follow-up data were available for 65 aneurysms in 62 patients in our retrospective analysis. Baseline population characteristics are outlined in Table 1.
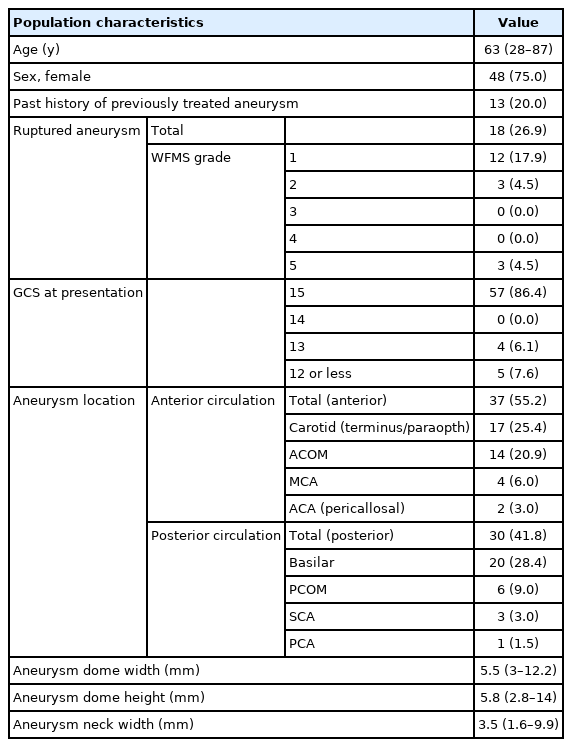
Baseline demographics and aneurysm location, size, and morphology
The median age was 63 (range 28–87) years, and most patients were female (75%). Eighteen (26.9%) ruptured aneurysms were included, most of which were World Federation of Neurosurgical Surgeons grade 1 presentations (12 of 18, 66.7%). Most aneurysms were in the anterior circulation (n=37, 55.2%). Three middle cerebral artery (MCA) bifurcation aneurysms were also included. The median aneurysm dome height was 5.8 mm (range 2.8–14 mm) with a median neck width of 3.5 mm (range 1.6–9.9 mm). Thirteen patients (20%) had undergone prior treatment for intracranial aneurysms. Three patients received 2 WEB devices each. In 1 of these patients, 2 WEB devices were deployed during the same procedure in distal pericallosal artery and anterior communicating artery (ACOM) aneurysms.
Table 2 outlines periprocedural antiplatelet use. Antiplatelet regimens varied and were dependent on operator preference, patient compliance, and the presence of antiplatelet resistance as determined by the VerifyNow P2Y12 assay (Accumetrics, San Diego, CA, USA). One patient was converted to Prasugrel after platelet function testing and high platelet reactivity unit values were noted on Clopidogrel. Eighteen patients who presented with ruptured aneurysms were not pre-medicated with antiplatelet agents. Failure of deployment was encountered in a single case of an unruptured 7 mm posterior inferior cerebellar artery aneurysm, which was subsequently converted to endovascular coiling during the procedure due to difficult aneurysm neck access precluding safe positioning of the WEB device. Adjunct coiling and/or stenting was performed in 14 cases (20.9%). Immediate complete angiographic occlusion was achieved in 88.1% (n=59) of cases (WOS A&B in 58 patients and mRROC RAY 3A in a single case in which coil embolization alone was performed).

Periprocedural antiplatelet use, procedural outcomes, and immediate angiographic occlusion
Clinical Outcomes
Table 3 outlines complications encountered, the need for retreatment, follow-up time, clinical outcome, and early/interim angiographic outcome in our cohort. Functional independence (mRS 0–2) at follow-up was achieved in 58 patients (93.5%); 13 patients who presented with ruptured aneurysms were functionally independent at clinical follow-up. Three patients had an mRS of 1 at follow-up; a single treated unruptured right posterior communicating artery aneurysm had a persistent third cranial nerve palsy at clinical follow-up and a second patient suffered a delayed stroke to an alternate vascular territory after treatment of the index right superior cerebellar artery aneurysm with mild residual deficit at follow-up. Treatment of an 8.3×6.3 mm ACOM aneurysm with a 6.2 mm neck was complicated by pericallosal artery wire perforation and acute SAH; however, this patient was functionally independent at follow up (mRS 0).
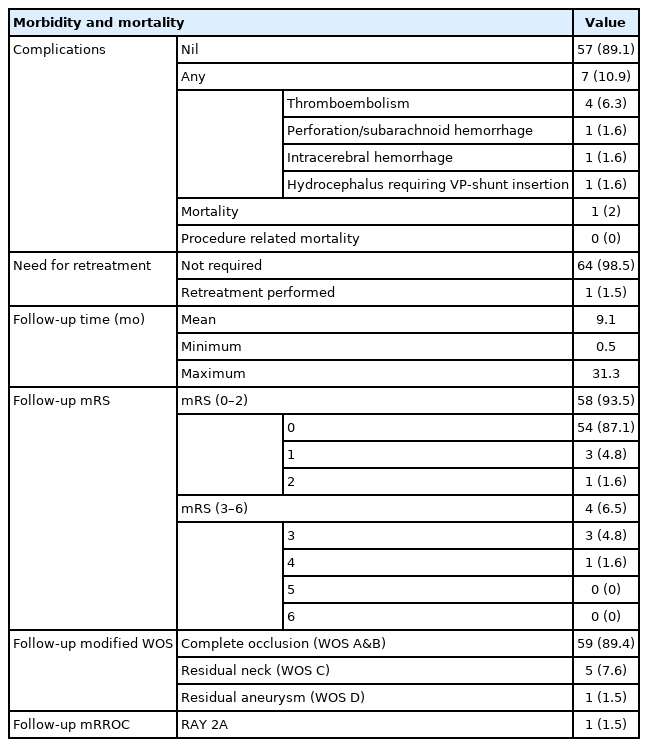
Complications, need for retreatment, follow up time, clinical outcomes, and early/interim angiographic outcomes
One patient with an unruptured 3×4 mm left ICA terminus aneurysm suffered an acute clinical deterioration post WEB deployment secondary to a large intraparenchymal hemorrhage distal to the treated aneurysm. The patient had previously had right MCA and right ICA aneurysms treated 6 weeks prior (with a WEB and coil embolization respectively) and had been on dual antiplatelet therapy after deployment of a right ICA stent during the first procedure. Additional left anterior temporal artery and right M1 aneurysms were treated during the same session. The exact cause of this was unknown and ultimately resulted in significant permanent neurological morbidity (mRS 5). Another patient with a treated wide-necked 7 mm basilar tip aneurysm subsequently died following the rupture of a separate untreated giant ACOM aneurysm several weeks after treatment (mRS 6).
Radiological Outcomes
A total of 62 patients with 65 aneurysms with a WEB device were followed up with multisequence MRI and non-contrast TOF MRA between 2 weeks and 31 months post-procedure. Fifty-nine of these had complete aneurysm occlusion (WOS A&B: 89.4%) and 1 remained patent (WOS D: 1.5%). Adequate occlusion was achieved in 1 patient with failed WEB deployment in which multiple soft Medtronic coils were used (modified Raymond–Roy occlusion RAY 3A) on their most recent follow-up imaging. There were initially 2 patients with WOS D occlusion and they both had identifiable sizing issues during deployment. Retreatment using stent-assisted coiling was successfully performed in 1 of these patients who went on to achieve WOS B on subsequent imaging. The second patient improved to WOS C on their most recent imaging.
DISCUSSION
Our results are comparable to a previously published case series with an overall technical success rate of 98.5%, with only a single patient showing an unfavorable angle that precluded safe device deployment. Pierot et al. [8] demonstrated a technical success rate of 96.4% with reported causes for failure including device protrusion into the parent vessel, lack of appropriate device sizing, and failure to deploy the device. Similarly, the WEB-IT trial reported a technical success rate of 98.7% quoting similar reasons [7]. Overall, our adequate occlusion rate was 90.7%, which is similar to international standards [5,8]. The WEB device can be combined with traditional coil embolization particularly if there is concern about daughter lobes or a point of recent rupture necessitating the need to secure the aneurysm dome prior to occluding the aneurysm neck.
Of 18 ruptured aneurysms, there was 1 mortality; and of the remaining 17 at mid-term follow-up, 14 achieved WOS A&B (82.4%), 2 were WOS C (11.8%), and 1 was WOS D (5.9%). This is comparable to the reported literature, as Youssef et al. [14], in a study involving 48 patients with ruptured IAs, reported adequate occlusion in 92.3% at a median follow up of 5.5 months, and Cortez et al. [15], in a study of 91 patients with ruptured IAs, demonstrated 80% adequate occlusion at a mean follow up of 3.4 months. A subsequent meta-analysis by Essibayi et al. [16] pooled 487 patients with 496 ruptured aneurysms treated with WEB, reporting an adequate occlusion rate of 87.3%. The single mortality in our series was unrelated to WEB deployment. The patient presented with a rupture of a second giant 19 mm ACOM aneurysm 1 month after treatment of a ruptured 7 mm wide-necked basilar tip aneurysm.
A second patient suffered a delayed large intraparenchymal hemorrhage with permanent morbidity (mRS of 5 at 3 months) after treatment of several aneurysms in a single session including deployment of an SL 5×3 WEB into a 5 mm left ICA terminus aneurysm and concomitant coiling of left anterior temporal artery and right M1 aneurysms.
The use of endosaccular coiling for many intracranial aneurysms gained acceptance following the ISAT trial after it demonstrated an increased disability-free survival at 7 years compared to neurosurgical clipping [3]. However, this trial was conducted many years ago and several novel techniques and devices have since been developed, further encouraging the use of minimally invasive treatments. In particular, these advances have made the endovascular treatment of wide-necked aneurysms safer with low periprocedural morbidity and mortality [5]. Pooled data from 15 uncontrolled studies reported complete or near-complete occlusion rates of 74.5% and retreatment rates of 5.8% with or without stent assistance after at least 6 months of angiographic follow-up [5]. Pierot et al. [17] demonstrated a retreatment rate of 9.3% at 2 years in a combined analysis of 3 prospective European trials, with the majority of patients requiring retreatment in their first year.
As an intrasaccular flow diverter, the WEB device allows the treatment of more complex wide-necked aneurysms which are less suitable for other endovascular devices. One-year retreatment rates are low, ranging from 6% [5] to 7.1% [8,17], and are similar to those treated with coiling (5.2%) [9]. Additionally, the WEB device can be used to treat aneurysms of differing geometry and locations given its range of shapes and sizes. Other benefits of the WEB device include shorter procedural times attributed to single-step treatment in most selected cases. Whether this translates into lower overall implant cost when compared to stent-assisted coiling is yet to be determined in the Australian context.
Wide-necked bifurcation aneurysms have traditionally been more difficult to treat endovascularly. A meta-analysis of 36 studies found that factors related to short-term angiographic obliteration include unruptured status, location in the anterior circulation, a medium neck (4–9.9 mm), use of newer-generation WEB, and treatment without additional devices [18]. Reported rates of 12-month complete occlusion rates after using coiling and stent-assisted coiling for the treatment of wide-necked aneurysms are 27.1% and 45.7%, respectively [19]. These results are inferior to rates of 54.8%, 53.8%, and 52.9% that have been reported when using the WEB device [6-8]. Stent-assisted coiling can offer high long-term complete aneurysmal occlusion; however, 12-month morbidity and mortality rates reported with its use in wide-necked aneurysms (7.5%) are considerably higher than that of coiling (1.5%) with WEB [19]. The multicenter Canadian-led RISE trial—a randomized controlled trial comparing intra-saccular flow diversion versus conventional management (surgical or endovascular) is currently underway and seeks to determine whether intravascular flow diversion leads to better long-term outcomes [20].
Known complications of the WEB device include failed deployment, thromboembolic events, and intracranial hemorrhage either from aneurysm rupture or vessel perforation. Goertz et al. [21] report a lower aspect ratio and an increased width to height ratio are significant risk factors for procedural complications. Our thromboembolism rate of 6.3% was lower than previously reported results, which range from 7.4% to 14.4% [5,7,8]. It is also within the reported thromboembolism rate in large coiling series (5.4% for unruptured aneurysms and 20.8% for ruptured aneurysms) [22,23]. Reported rates of procedural intracranial hemorrhage with WEB are low. WEB-IT and Pierot et al. [8] reported intracranial hemorrhage rates of 1.2% and 0.6%, respectively [7]. Our results are similar, and these are comparable to those published with coiling [22,23]. Long-term morbidity is also low with a reported 12-month procedure-related morbidity rate of 1.3%.
Like previous studies, we encountered no periprocedural or postprocedural deaths suggesting that the mortality risk associated with WEB is low. This high safety profile is likely to continue into the long-term, with WEB-IT and Pierot et al. [8] reporting 12-month procedure-related mortality rates of 0% and 1.3%, respectively [7]. To our knowledge, delayed aneurysm rupture following treatment with WEB has not been reported.
Limitations
The present analysis is limited by its retrospective nature and potential for patient selection bias. The small cohort of patients is heterogeneous with aneurysms varying in location, morphology, and clinical presentation limiting generalizability. Furthermore, the short interval for follow-up for many of these patients may not account for delayed neck recanalization. Further long-term follow-up will be required. While all patients were followed up with MRI as per our standard post embolization protocol, it remains to be seen whether MRI is the most appropriate and accurate method in which to assess aneurysm occlusion after WEB deployment. While interobserver reproducibility was excellent for contrast-enhanced (CE)-MRA (κ=0.92; 95% confidence interval [95% CI], 0.76–1.00) and moderate (κ=0.59; 95% CI, 0.30–0.88) for 3D TOF, Timsit et al. [24] reported low sensitivity on both CE-MRA and 3D TOF MRA for remnant detection, with 3 out of 4 recurrences not detected on MRA and only fair inter-modality agreement with digital subtraction angiography (DSA). Similarly, Mine et al. [25] reported that 40% of aneurysm remnants were not detected on CE-MRA. While MRA remains the standard for screening, like flow diversion and stent placement, 6-month or 1-year delayed DSA should be considered the gold standard for follow-up but is not necessarily practical due to the risks associated with more invasive testing. Despite these limitations, this study demonstrates that the use of the WEB device to treat intracranial aneurysms in Australia produces similar results to those seen internationally. This is particularly significant given the recent rise in use of WEB devices in the Australian population.
CONCLUSION
Early results following the use of WEB devices in Australia demonstrate safety and adequate aneurysm occlusion comparable to international literature.
Acknowledgements
All investigators freely volunteered their time towards this project. Department of Radiology, Austin Health, Melbourne, VIC, Australia. Department of Radiology, Monash Health, Melbourne, VIC, Australia. Department of Radiology, St. Vincent’s Health, Melbourne, VIC, Australia. Department of Radiology, Canberra Hospital, ACT Health, Canberra, NSW, Australia. Department of Radiology, Royal Hobart Hospital, Hobart, TAS, Australia. Department of Radiology, Royal North Shore Hospital, Sydney, NSW, Australia.
Notes
Fund
None.
Ethics Statement
Low Negligible Risk Study, retrospective, approved by local institutional review board. As specific patient information such as age or sex is not included, Informed consent for publication is not required.
Conflicts of Interest
The authors have no conflicts to disclose.
Author Contribution
Concept and design: HA. Analysis and interpretation: JG, JM, and HA. Data collection: JG, YR, AL, DN, JH, DK, DT, SL, RMFB, JR, LS, RC, WC, AJ, DMB, and HA. Writing the article: JG and JM. Critical revision of the article: JG, JM, MF, YR, AL, DN, JH, DK, DT, SL, RMFB, JR, LS, RC, WC, AJ, DMB, and HA. Final approval of the article: JM and HA. Statistical analysis: JG, MF, and HA. Overall responsibility: HA.