Parent Artery Complex Coil Protection for Side-Branched Wide-Neck Aneurysms
Article information

Abstract
This study aimed to validate the usefulness of parent artery complex coil protection for the treatment of wide-neck, side-branched, and ruptured aneurysms. A microcatheter was first introduced into the aneurysmal sac, and another microcatheter was introduced into the parent artery or near the orifice of the branch artery. A framing coil was deployed partially from the first microcatheter, and a protection coil was deployed from the second microcatheter to prevent protrusion of the first framing coil to the parent artery and side branches. After the first framing coil insertion, the protection coil was withdrawn to confirm the stability of the framing coil and blood flow. The procedures with this technique were successful for 3 patients. Parent artery complex coil protection can be an effective and safe coil embolization technique for the preservation of parent and side branch arteries and an alternative method for emergent ruptured cases.
INTRODUCTION
Coil embolization for wide-necked and branch-incorporated aneurysms is still technically difficult and various techniques have been developed [1-5]. These techniques have enabled coil embolization of aneurysms with complex configurations; however, some lesions are not amenable to treatment due to acute angulation of branches and a small artery caliber. In addition, the stent-assisted technique has been prohibited for ruptured aneurysm cases.
For challenging cases, there are reports on coil protection techniques in the literature [6-8]. We have developed a new technique, called the parent artery complex coil protection technique, which uses a protective complex coil for similarly difficult cases. In this study, we retrospectively evaluated the safety and validity of the parent artery complex coil protection technique.
Clinical Menifestation
Three cases of aneurysms were evaluated in this study: 2 were ruptured aneurysms and the other showed imminent rupture signs of third cranial nerve palsy. They were treated using the endovascular procedure with the parent artery complex coil protection technique. We chose not to use intracranial stents in these emergency cases because we could not start the preoperative antiplatelet administration. The procedures and techniques were successful in all the cases. There were no related complications, such as thrombosis or bleeding. Only 1 patient had a postoperative spotty hyperintense area on diffusion-weighted imaging (DWI) but without symptoms. The postoperative outcomes of all the cases were good.
Technical Approach
All procedures were performed under general anesthesia. The femoral artery was punctured in the inguinal region on either side. Using an 8 Fr long sheath in all patients, an 8 Fr RoadMaster 80 cm (Goodman, Aichi, Japan) was placed in the common carotid artery on the treatment side as a guide. For the inner catheter of the 6 Fr Cerulean DD6 118 cm (Medikit, Tokyo, Japan), a 4.2 Fr Fubuki 130 cm (Asahi Intecc, Aichi, Japan) was used, and a head-shaped DD6 was advanced into the C3/4 portion of the internal carotid artery.
We performed the parent artery complex coil protection technique as follows. For step 1, the first microcatheter was introduced into the aneurysmal sac, but the attempt to put the first framing coil failed due to coil protrusion (Fig. 1A). For step 2, the second microcatheter was introduced into the parent artery or near the orifice of the branch artery. A framing coil was partially deployed from the first microcatheter, and a protection complex coil was deployed from the second microcatheter to prevent the first framing coil from protrusion to the parent artery and side branches. The entire length of the framing coil was successfully inserted into the aneurysm sac with the help of a protective coil (Fig. 1B). For step 3, the protection coil was gently withdrawn to confirm the stability of the framing coil and blood flow after the first framing coil insertion (Fig. 1C). For step 4, the coil embolization was continued from the first microcatheter till the end, and the protection coil was essentially inserted into the aneurysmal sac.
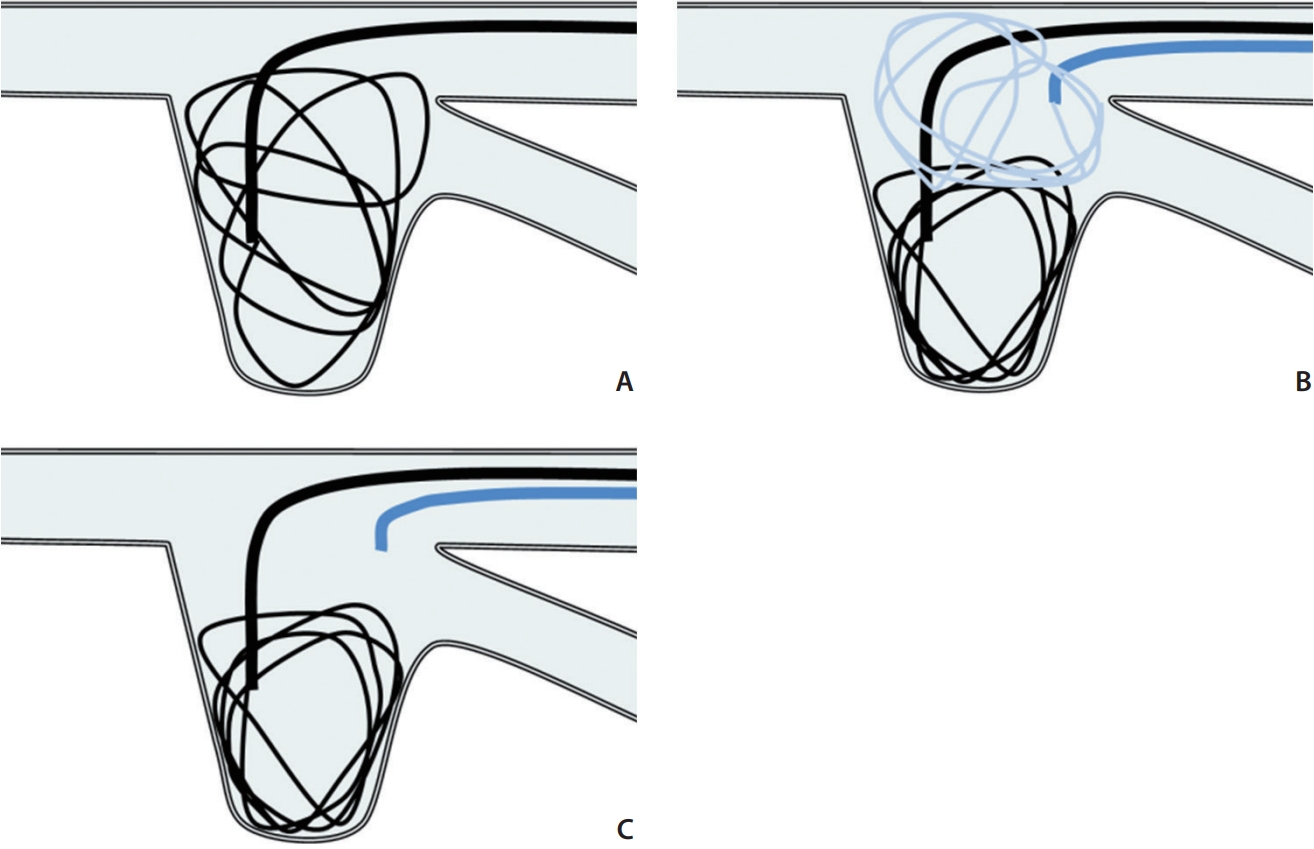
Schematic of the parent artery coil protection technique for the side-branched aneurysm. (A) Because of the wide neck, the first framing coil protrudes into the side branch and parent artery. (B) The first framing coil is inserted into the aneurysm sac and is stable with a protective coil from the second microcatheter. (C) After withdrawing the protective coil, the stability of the framing coil should be confirmed.
CASE REPORT
Case No. 1
An 84-year-old female patient had right third cranial nerve palsy and was urgently admitted for treatment of a right internal carotid-posterior communicating artery aneurysm. Coil embolization was performed the day after admission. Digital subtraction angiography (DSA) revealed a wide-neck internal carotid-posterior communicating artery aneurysm, which was 6 mm in dome height and 5 mm in neck width. The aneurysm aspect ratio was 1.2. The posterior communicating artery (Pcom) was incorporated into the aneurysm neck (Fig. 2A, B). We initially attempted to treat the aneurysm using a simple technique with the Target 360 XL Soft 5 mm×15 cm (Stryker-Neurovascular, Kalamazoo, MI, USA) from the first microcatheter in the aneurysmal sac but failed to preserve the Pcom due to coil protrusion. We introduced the second microcatheter into the internal carotid artery just in front of the aneurysm and attempted parent artery complex coil protection with the Target 360 Ultra 4 mm×8 cm. The protection coil size (4 mm) was decided by the total length of the internal carotid artery diameter (2.5 mm) and the Pcom diameter (1.5 mm). First, the framing coil was partially inserted into the sac without protrusion. After the protection coil was partially inserted at the aneurysmal neck near the Pcom, the first framing coil was inserted completely, and optimal framing was achieved (Fig. 2C). The stability of the framing coil and preservation of the incorporated branch were confirmed after withdrawing the protection coil, which was also inserted into the sac as a filling coil. Finally, 5 coils with a total length of 41 cm were inserted into the aneurysm (Fig. 2D, E). Magnetic resonance DWI images at 7 days after the procedure showed spotty hyperintense areas, but there were no symptoms (Fig. 2F).
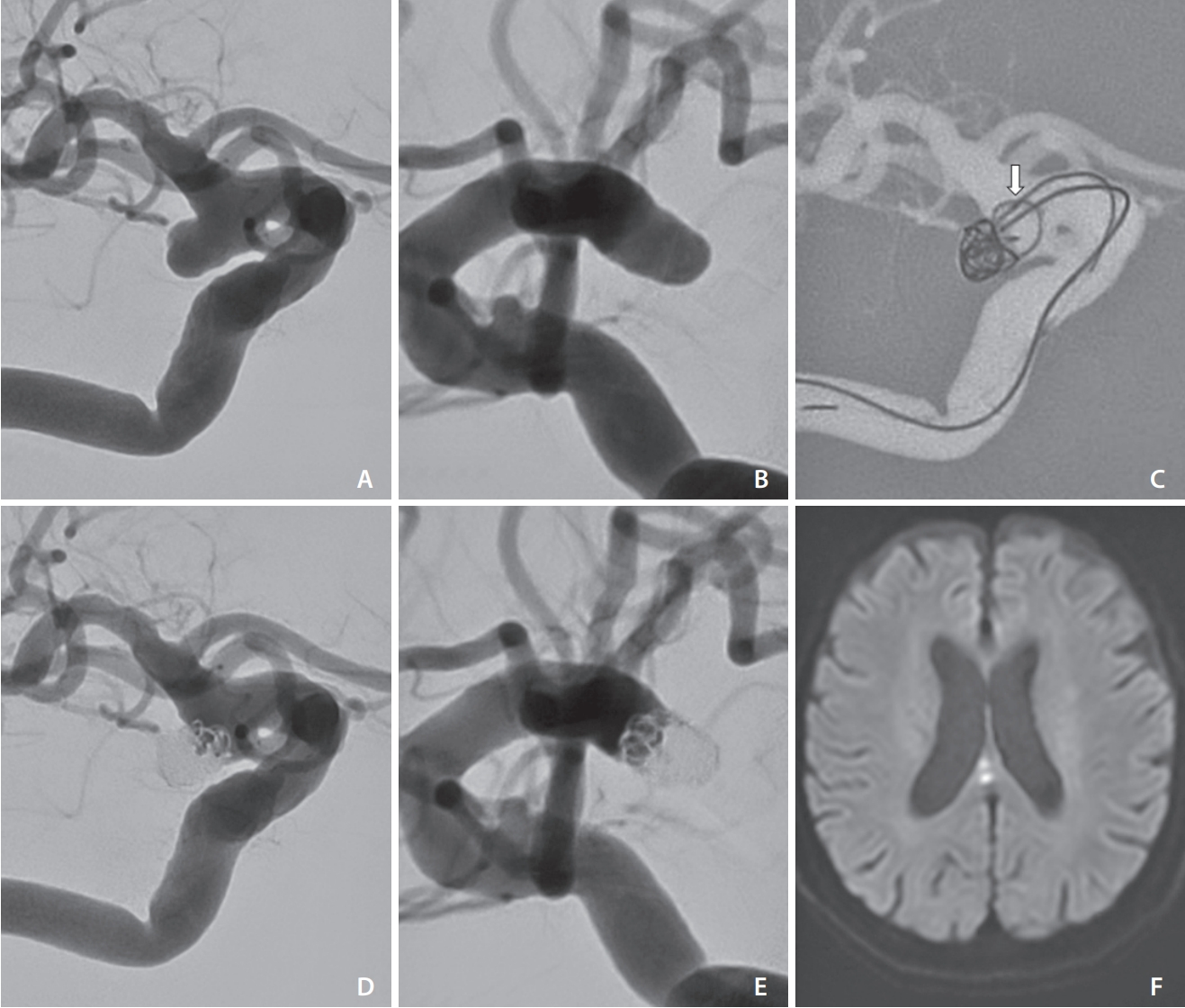
(A, B) Working views of the right internal carotid angiograms show a wide neck IC-PC aneurysm. (C) First framing coil was inserted with the parent artery coil protection from the second microcatheter (white arrow). (D, E) Right internal carotid angiograms after the procedure show good preservation of the posterior communicating artery. (F) Postoperative magnetic resonance DWI shows spotty hyperintense areas, but there were no symptoms. IC-PC, internal carotid-posterior communicating artery; DWI, diffusion-weighted imaging.
Case No. 2
A 76-year-old male patient was urgently admitted for a Hunt and Kosnik Grade 5 subarachnoid hemorrhage caused by rupture of the basilar artery (BA) tip aneurysm, and emergency coil embolization was performed the day after admission.
DSA revealed a very wide-neck BA tip aneurysm, which was 11 mm in dome height and 7 mm in neck width. The aneurysm aspect ratio was 1.57. The bilateral posterior cerebral arteries were incorporated into the aneurysm neck (Fig. 3A, B). Stent-assisted coiling could not be performed because of the rupture. Therefore, we initially attempted to treat the aneurysm using a simple technique and a standard double catheter technique but failed to make the first framing because of the strong inflow/outflow jet.
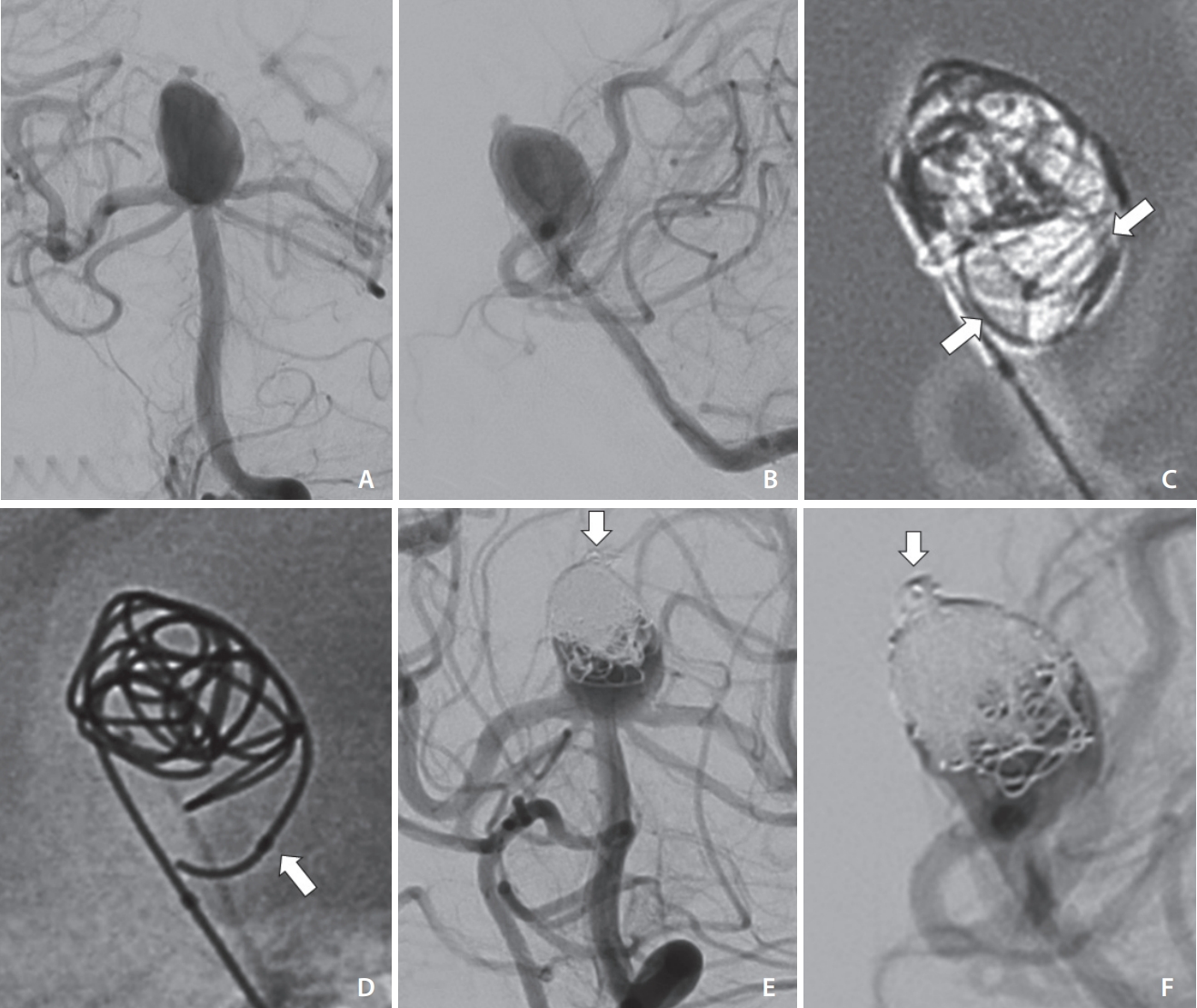
(A, B) Working views for the left vertebral angiograms show a very wide-neck BA tip aneurysm. (C) First framing coil was inserted with the protection of the coil loops (between white arrows) from the second microcatheter. (D) After withdrawing the protection coil, the stability of the framing coil was confirmed. The white arrow shows the second microcatheter tip. (E, F) Left vertebral angiograms after the procedure show good preservation of the bilateral PCA and SCA. The white arrows show good obliteration of the ruptured bleb. BA, basilar artery; PCA, posterior cerebral artery; SCA, superior cerebellar artery.
Therefore, we introduced the first microcatheter in the center of the aneurysmal dome, followed by the second microcatheter at the BA tip with 1 turning in the aneurysmal dome (Fig. 3D).
The protection coil, the Target XL 360 Soft 7 mm×20 cm, was partially inserted from the second microcatheter using the parent artery complex coil protection technique to make the framing at the upper side of the aneurysmal dome after inserting some loops of the framing coil, the Target XL Helical 6 mm×20 cm (Fig. 3C). According to the total length (12.5 mm) of the dome height (11 mm) and posterior cerebral arteries diameter (1.5 mm), the protection coil size (7 mm) was decided after partially inserting the framing coil (6 mm). The first framing coil was inserted completely under the protection coil, and the stability of the framing coil was confirmed after withdrawing the protection coil (Fig. 3D). With this coil protection, 7 coils, with a total length of 84 cm, were inserted into the aneurysm (Fig. 3E, F). Magnetic resonance DWI image at 8 days after the procedure showed no ischemic area.
DISCUSSION
Owing to improvements in various protective devices and adjunctive techniques, including balloon remodeling and stent protection, endovascular treatment for previously ineligible aneurysms with difficult configurations has been recently achieved [9]. However, anatomical complexities such as acutely angled incorporated branches and extreme vessel tortuosity sometimes makes the use of these techniques difficult [10].
Multiple catheter or catheter-assisted techniques can be available when a balloon or stent cannot be inserted into the side branched artery because of the narrow diameter and acute turnout angle [5,11]. There are reports on the validity of coil protection techniques that prevent the protrusion of a framing coil into the parent artery and incorporated branch artery [6-8]. However, a similar coil protection technique that uses a large-diameter complex coil in the parent artery for the neck coverage of small aneurysmal coil embolization has been described before [12].
Parent artery complex coil protection has advantages similar to those of coil protection techniques that have already been reported [6-8]. First, there is no stasis of blood flow through the parent arteries and side branches. Second, this coil protection technique allows free control of microcatheters and repetitive modifications of the first framing coil for an optimal shape. In addition, this technique can be changed to a double catheter technique with a microcatheter for the protection coil, and the protection coil can be used as a filling coil after stabilizing the framing coil. The coil protection technique does not require antiplatelet therapy after the procedure. Therefore, these techniques are helpful for the treatment of ruptured aneurysms.
The parent artery complex coil protection technique is significantly different from the previously reported techniques in terms of microcatheter position for the protection coil and the choice method of the protection coil size. The microcatheter for the protection coil is simply put at the parent artery. So the position is not needed to be strict and this technique is easier than the previous techniques [6-8]. The behavior of the complex coil is randomly performed in the large vessel space by repetitive insertions. Then, as in the representative cases, the protection coil size is generally calculated and decided by the preservation space defined by the aneurysm size, the parent artery diameter, and the incorporated artery diameter. The protection coil is not inserted in the branch, so blood flow may not be significantly reduced.
Though the microcatheter positioning of the parent artery complex coil protection technique is relatively easy, for the success of this technique, it is important to optimize the microcatheter shape for effective protection against the framing coil according to the situation (Fig. 1). In addition, microcatheter control and repetitive protection coil insertion may be needed. If the framing coil protrudes after withdrawal of the protection coil, the framing coil should also be partially withdrawn and remodeled for optimal frame shape. Subsequently, after the protection coil is repositioned and inserted partially once again, the framing coil is inserted until the optimal framing is achieved.
Parent artery complex protection has some problems, such as the risk of intraoperative thrombosis, coil tangling, and stretching of coils. However, a previous report showed that intraoperative thrombosis did not occur with the coil protection technique due to the preservation of the blood flow during the procedure [8]. During the parent artery complex coil protection technique, the protection and framing coils are deployed individually in separate areas. Therefore, there is a low risk of coil tangling (Fig. 1).
CONCLUSION
There are only 3 cases in this study and this technique may not be the first choice for cerebral aneurysm coil embolization; however, it can be an effective and alternative method for ruptured cases and unsuitable cases when using a microballoon catheter or an intracranial stent. In addition, this technique might be simpler than the previously reported techniques in terms of microcatheter position and the choice method of the protection coil size.
SUPPLEMENTARY MATERIALS
The remaining case presentation can be found online at https://doi.org/10.5469/neuroint.2022.00136.
Notes
Fund
None.
Ethics Statement
Written informed consent was obtained from the patient for publication of this case report and accompanying images. The relevant Institutional Review Board approved this retrospective study.
Conflicts of Interest
The authors have no conflicts to disclose.
Author Contributions
Concept and design: KS. Analysis and interpretation: HA, SJ, HS, and KS. Data collection: KS. Writing the article: KS. Critical revision of the article: TK and KS. Final approval of the article: KS. Statistical analysis: KS. Overall responsibility: KS.