Strong Contrast Stagnation of Unilateral Vertebral Artery on Three-Dimensional Black Blood-Enhanced MRI Predicts Acute Medulla Infarction
Article information

Abstract
Purpose
This study aimed to evaluate angiographic and contrast enhancement (CE) patterns on three-dimensional (3D) black blood (BB) contrast-enhanced MRI in patients with acute medulla infarction.
Materials and Methods
From January 2020 to August 2021, we retrospectively analyzed stroke 3D BB contrast-enhanced magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) findings of patients visiting the emergency room for symptom evaluation of acute medulla infarction. In total, 28 patients with acute medulla infarction were enrolled in this study. Four types of 3D BB contrast-enhanced MRI and MRA were classified as follows: 1=unilateral contrast-enhanced vertebral artery (VA)+no visualization of VA on MRA; 2=unilateral enhanced VA+hypoplastic VA; 3=no enhanced VA+unilateral complete occlusion of VA; 4=no enhanced VA+normal VA (including hypoplasia) on MRA.
Results
Of the 28 patients with acute medulla infarction, 7 (25.0%) showed delayed positive findings after 24 hours on diffusion-weighted imaging (DWI). Of these patients, 19 (67.9%) showed CE of the unilateral VA on 3D BB contrast-enhanced MRI (type 1 and 2). Of the 19 patients with CE of VA on 3D BB contrast-enhanced MRI, 18 showed no visualization of enhanced VA on MRA (type 1), and 1 showed hypoplastic VA. Of the 7 patients with delayed positive findings on DWI, 5 showed CE of the unilateral VA and no visualization of the enhanced VA on MRA (type 1). Symptom onset to door time or initial MR check time was significantly shorter in the groups with delayed positive findings on DWI (P<0.05).
Conclusion
Unilateral CE on 3D BB contrast-enhanced MRI and no visualization of the VA on MRA are related to the recent occlusion of the distal VA. These findings suggest that the recent occlusion of the distal VA is related to acute medulla infarction, including delayed visualization on DWI.
INTRODUCTION
Posterior circulation infarction, which consists of about 20%–25% of all ischemic strokes, includes any infarction within the vertebrobasilar arterial system [1]. Brainstem infarction accounts for 48% of all posterior circulation infarctions, and 7% of brainstem infarctions are medulla infarctions [1,2]. Among the 5 subtypes developed in the Trial of Org 10172 in Acute Stroke Treatment, large-artery atherosclerosis is known to be the most common mechanism (34.5%) for medulla infarction [3].
Diffusion-weighted imaging (DWI) is a useful diagnostic tool for acute infarction, with a sensitivity of 88% and specificity of 95% [4]. However, in DWI taken within 24 hours from symptom onset, high rates of false-negative results (31%) have been reported in posterior circulation infarction patients [5]. Compared to patients with anterior circulation infarction (2%), this is a high number [5]. Since medulla infarction is a life-threatening disease, early diagnosis and initial aggressive treatment are important. To improve the weaknesses of DWI, a new imaging tool should be considered for diagnosing medulla infarction.
Three-dimensional (3D) black-blood (BB) contrast-enhanced magnetic resonance imaging (MRI) suppresses the signal of flowing blood and enhances static tissue from the vessel wall [6,7]. Therefore, since 3D BB contrast-enhanced MRI can distinguish the arterial wall from the lumen, intravascular lesions such as atherosclerosis and thromboembolic occlusions can be identified better than other modalities used in neurovascular imaging [8,9]. Since vessel wall lesions are the major cause of cerebral infarction, 3D BB contrast-enhanced MRI may overcome the diagnostic delay of DWI and be helpful in the early detection of stroke [9].
To our knowledge, there have been no studies associating distal vertebral artery (VA) contrast enhancement (CE) on 3D BB contrast-enhanced MRI with acute medulla infarction. We categorized the enrolled patients into 4 types according to whether MR angiography (MRA) findings suggested occlusion, hypoplasia, or normal and whether distal VA CE was shown or not. The aim of this study was to evaluate the imaging findings of 3D BB contrast-enhanced MRI in patients with acute medulla infarction.
MATERIALS AND METHODS
Patients
Our institutional review board approved this retrospective study protocol, and the requirement for informed consent was waived for the review of patient medical records and images. From January 2020 to August 2021, we retrospectively reviewed stroke MR images with 3D BB contrast-enhanced MRI and MRA imaging of patients visiting the emergency room for the evaluation of acute brain infarction. We selected patients with initial or delayed positive DWI findings of the medulla and neurological symptoms. The exclusion criteria were as follows: (a) MR examination 48 hours after symptom onset; (b) evidence of vertebral dissection or vasculitis; (c) slow-flowing artifact or incomplete suppression of the VA lumen on 3D BB contrast-enhanced MRI; (d) any patient who had images of insufficient quality for reliable evaluation on 3D BB contrast-enhanced MRI or MRA; and (e) complete or severe stenosis of the proximal VA (V1–V3 segment) or no visualization of bilateral VA on MRA.
MRI Procedure
MR examination was performed using an Achieva 3.0-T MRI scanner (Philips Healthcare) with a 16-channel head coil. MRI for ischemic symptom evaluation was performed after an initially non-enhanced brain computed tomography scan to rule out intracranial hemorrhage. Our MR protocol included the following sequences: (a) DWI; (b) 3D time-of-flight MRA of the intracranial arteries; (c) susceptibility-weighted imaging (SWI); (d) 3D BB contrast-enhanced MR of the whole brain; (e) contrast-enhanced carotid MRA; and (f) fluid attenuated inversion recovery imaging.
This protocol has been previously described [8,10,11]. 3D BB contrast-enhanced MRI was performed using volumetric isotropic turbo spin-echo acquisition (Philips Healthcare) in the coronal plane (slab thickness=40 mm) for flow suppression. We used the improved motion-sensitized driven-equilibrium method, which suppresses enhanced signals in blood vessels [12,13]. Acquisition parameters for improved motion-sensitized driven-equilibrium– volumetric isotropic turbo spin-echo acquisition images were as follows: repetition time/echo time=450.0/22.4 ms, flip angle=90°, echo train=26, sensitivity encoding=2, field of view=256 mm×256 mm, matrix=256×256, 1-mm slice thickness and no gap, and scan time=35–38 seconds. Gadoterate meglumine (0.1 mmol/kg body weight; Dotarem; Guerbet) was injected as a bolus intravenously in all patients. BB contrast-enhanced MR was performed approximately 5 minutes after contrast injection. After image acquisition in the sagittal plane, the axial and coronal planes were reconstructed. Also, all patients underwent DWI for evaluation of new lesions or progression of a previous lesion within 48 hours after admission.
Clinical Data Analysis
Clinical data of the included patients, including basic demographics and risk factors for atherosclerosis, namely diabetes, hypertension, dyslipidemia, current smoking, and a history of coronary disease, were recorded.
MRI Analysis
All MR images, including 3D BB contrast-enhanced MRI and MRA, were reviewed retrospectively by 2 neuroradiologists (with 30 years and 16 years of experience, respectively) blinded to the clinical information of each patient and the purpose of this study. Two neuroradiologists analyzed the imaging quality, flow-related artifacts, pattern of CE, geometry of the VA, and location of acute infarction on DWI. They assessed the image quality by consensus. Poor imaging quality was defined as an ill-defined visualization of the VA or impossible analysis due to motion artifacts or incomplete coverage. Patients with poor image quality were excluded from the final analysis.
They analyzed whether MRA findings of both distal VA suggested occlusion, hypoplasia, or normal. VA hypoplasia was defined as a diameter with a difference of more than 2 mm [14]. In addition, enhancement of the VA lumen on 3D BB contrast-enhanced MRI was classified as follows: complete unilateral CE of the vessel lumen versus no CE. Target appearance with peripheral or partial CE and central BB lumen was defined as no CE due to different flow velocities and/or slow flow effects. The target appearances were excluded from the study. The length of the CE was graded as either short, referring to a lesion less than 10 mm, or long, which denoted a lesion >10 mm.
Four types of 3D BB contrast-enhanced MR and MRA were classified as follows: 1=unilateral contrast-enhanced VA+no visualization of VA on MRA; 2=unilateral enhanced VA+hypoplastic VA; 3=no enhanced VA+unilateral complete occlusion of VA; and 4=no enhanced VA+normal VA (including hypoplasia) on MRA (Fig. 1A–D).
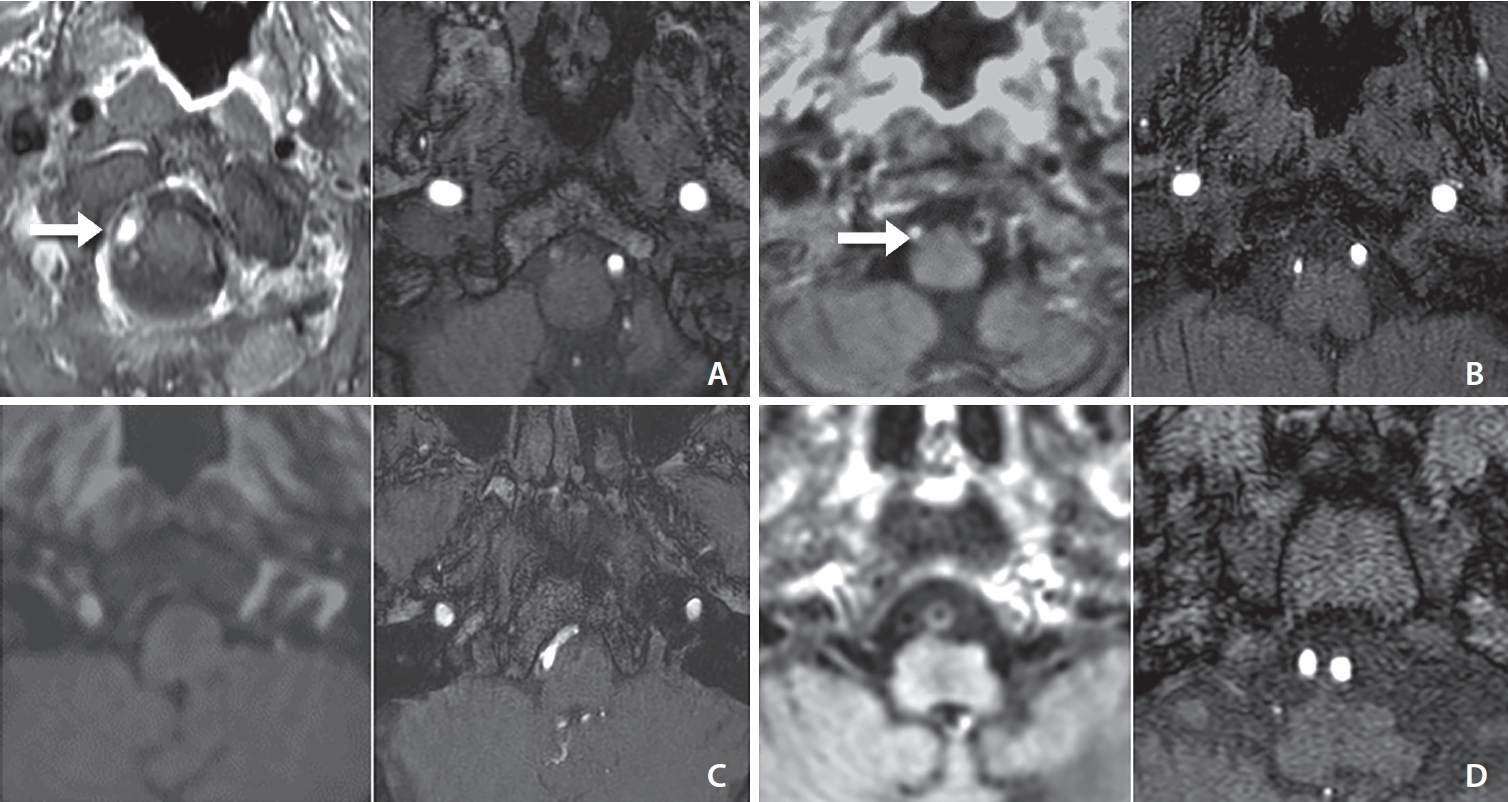
Four types of asymmetrical vertebral artery (VA) geometry on black blood enhanced manetic resonance (MR) and MR angiography (MRA). (A) Type 1=unilateral contrast-enhanced VA (arrow)+no visualization of VA on MRA. (B) Type 2=unilateral contrast-enhanced VA (arrow)+hypoplastic VA. (C) Type 3=no enhanced VA+unilateral complete occlusion of VA. (D) Type 4=no enhanced VA+normal VA (including hypoplasia) on MRA.
Acute medulla infarction is defined as the detection of a hyperintense signal on a DWI trace with an associated signal decrease on the apparent diffusion coefficient map. Positive DWI lesions and the location of infarctions were attained through consensus interpretation by 2 experienced neuroradiologists. Delayed positive findings were defined as negative lesions on the initial DWI, although patients had typical symptoms related to medulla infarction and positive lesions on follow-up DWI within 48 hours.
Statistical Analysis
All statistical analyses were performed with SPSS for Windows (version 23.0; IBM Corp.). Descriptive statistics are reported as numbers of patients and percentages. Categorical variables were coded numerically. The unpaired 2-tailed Student’s t-test and chi-squared test were used for statistical analyses. P-values of less than 0.05 were considered statistically significant.
RESULTS
During the study period, 34 patients with acute medulla infarction on DWI were enrolled. Of these patients, 2 were excluded from this study due to symptom onset 48 hours after the imaging study, 2 due to VA dissection, and 2 due to incomplete vessel suppression by slow flow. Twenty-eight patients (19 males, median age 68.5 years) were finally enrolled in this study. The demographic data of the patients are presented in Table 1.
The demographic data of the patients (n=28)
The imaging findings of 3D BB contrast-enhanced MRI and MRA in patients with acute medulla infarction are shown in Table 2. Of these patients, 19 (67.9%) showed CE of the unilateral VA (types 1 and 2). Of the 19 patients with CE of VA on 3D BB contrast-enhanced MRI, 18 showed no visualization of enhanced VA on MRA (type 1) and 1 showed hypoplastic VA (type 2). Eighteen patients with a type 1 lesion had ipsilateral medulla infarction (Fig. 2A–D).
Imaging findings of 3D BB contrast-enhanced MRI and MRA in patients with acute medullary infarction

A middle aged patient with left extremity weakness. (A) Initial diffusion-weighted imaging showing an acute infarction in the right lateral medulla (arrow). (B) Manetic resonance (MR) angiography shows no visualization of the right vertebral artery (VA) and faint visualization of the distal VA (arrow). (C) Axial 3-dimensional black-blood contrast-enhanced MR imaging (MRI) showing strong enhancement of the right VA (arrow). Note the black lumen of the left VA (asterisk). (D) Coronal reformatted contrast-enhanced MRI showing a long segment and strong contrast stagnation of the right VA (arrows).
Of the patients with acute medulla infarction, 7 (25.0%) showed negative findings on initial DWI and delayed positive findings after 48 hours on DWI. Of the 7 patients with delayed positive findings on DWI, 5 showed CE of the unilateral VA on 3D BB contrast-enhanced MRI and no visualization of the VA on MRA (type 1) (Fig. 3A–E), and 2 showed normal VA MRA and no CE on BB (type 4).
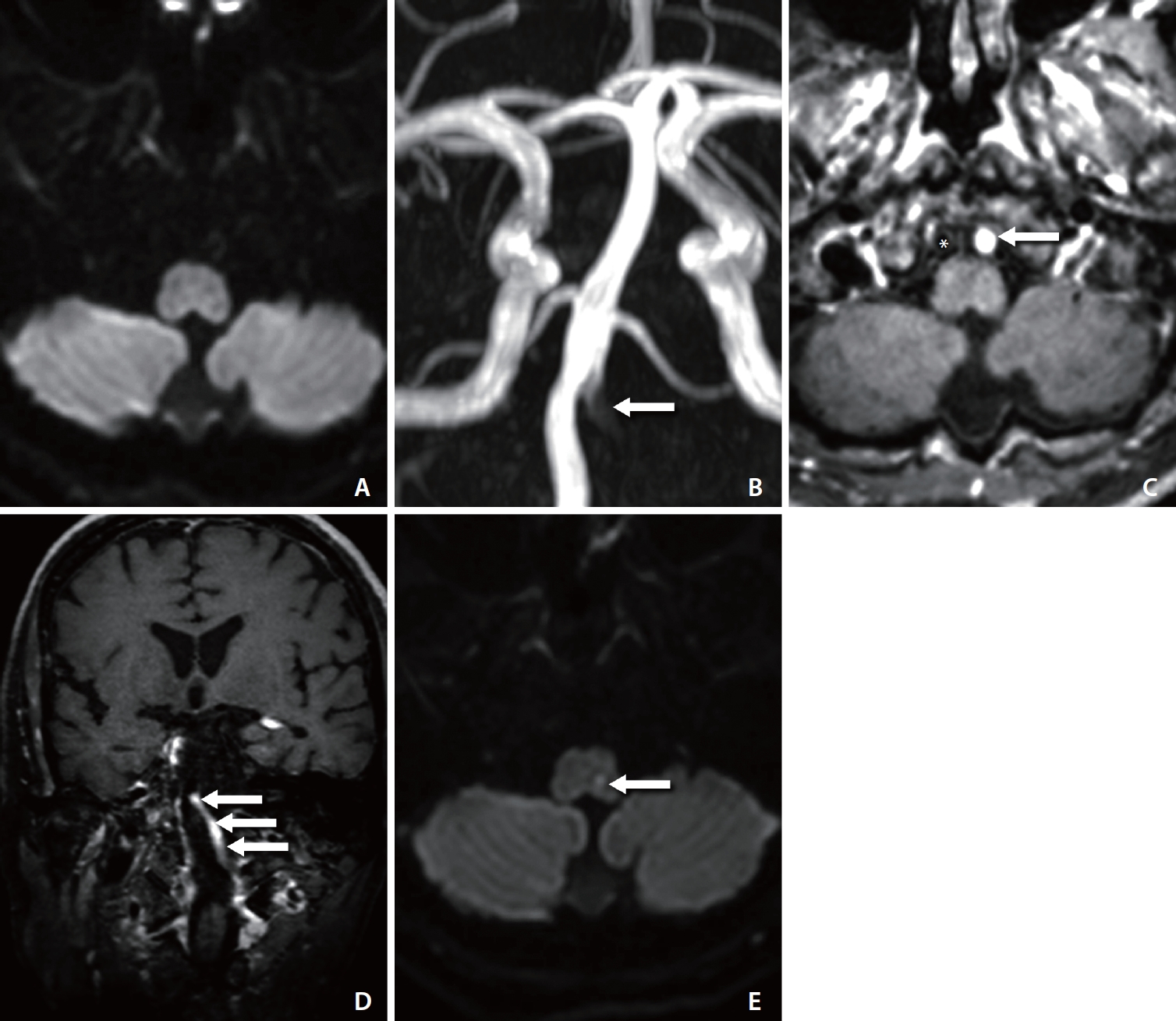
A middle aged patient with acute headache and dizziness. (A) Initial diffusion-weighted imaging (DWI) does not show abnormal signal intensity. (B) Manetic resonance (MR) angiography shows no visualization of the left vertebral artery (VA) and faint visualization of the distal VA (arrow). (C) Axial 3-dimensional black-blood contrast-enhanced MR imaging (MRI) showing strong enhancement of the left VA (arrow). Note the black lumen of the right VA (asterisk). (D) Coronal reformatted contrast-enhanced MRI showing a long segment and strong contrast stagnation of the left VA (arrows). (E) DWI 1 day later showing focal diffusion restriction in the left medulla (arrow).
Of 18 patients with a type 1 lesion, 5 (27.8%) had delayed positive findings on DWI after admission. The associated factors between a type 1 lesion and delayed positive findings on DWI are shown in Table 3. Symptom onset to door time or initial MR check time was significantly shorter in the groups with delayed positive findings on DWI (P<0.05).
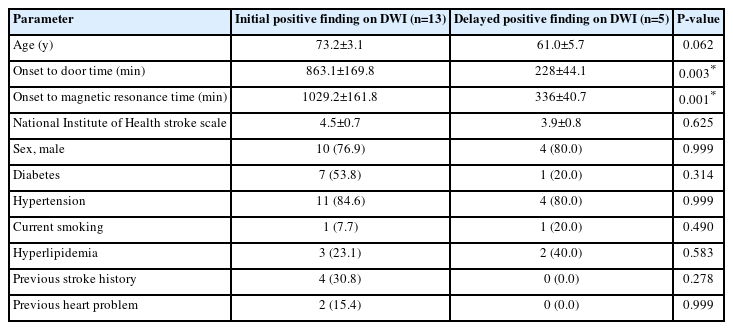
Association between type 1 lesion (n=18) and delayed positive findings on DWI
DISCUSSION
This study examined 3D BB contrast-enhanced MRI and MRA patterns of patients with acute medulla infarction. Eighteen patients (64.3%) had unilateral CE on 3D BB contrast-enhanced MRI and no visualization on MRA, which we classified as type 1. Among 7 patients (25%) whose DWI images showed delayed positive findings after 48 hours, 5 showed a type 1 pattern on initial 3D BB contrast-enhanced MRI and MRA. Early MR examination after symptom onset with acute medullar infarction was associated with initial negative findings and delayed positive findings on DWI.
Medulla infarction, a condition consisting of posterior circulation infarctions, is caused by vascular changes in the vertebrobasilar arterial system. In a large study of 142 patients with medulla infarction, large-artery atherosclerosis was the most common etiology of medulla infarction (34.5%) [3]. Among all the patients with medulla infarction, 36 (25.4%) showed VA occlusion and 38 (26.7%) showed significant stenosis (≥50%) of the VA as the blood stagnation of the VA results in hemodynamic brain ischemia, early diagnosis and treatment are significantly important to achieve good prognosis. However, DWI in patients with posterior circulation infarction has a critical limitation: a high false-negative rate (31%) within 24 hours [5]. In our study, overall delayed positive findings on DWI in patients with acute medullar infarction was 25.0%. Of these patients, 5 had unilateral CE of the target VA and no visualization of VA on MRA (type 1 lesion).
BB MR sequences selectively suppress signals from flowing blood while maintaining a high signal in surrounding static structures, providing a clear assessment of various intravascular lesions, including atherosclerotic plaque, thromboembolism, vasculitis, and dissection [6]. BB-enhanced MRI is a very informative tool for finding intra-arterial thrombi in patients with acute infarction, both in the anterior and posterior circulation, and it is more accurate than that of a susceptibility vessel sign on SWI [8,11]. Previous studies have shown that 3D BB contrast-enhanced MRI can identify intracranial arterial steno-occlusive lesions with higher sensitivity and specificity than conventional angiographic modalities [6]. The main finding of 3D BB-enhanced MRI in acute stroke patients is strong CE due to contrast stagnation in the front and rear of the thrombus or steno-occlusive lesions in the intracranial occlusion site [8,15,16]. Chung et al. [11] reported that the sensitivity of BB-enhanced MRI by strong CE for detection of vessel occlusion in patients with posterior circulation stroke was significantly higher than that of susceptibility vessel sign on SWI. We focused on the strong CE of the asymmetrical VA and the acute infarction of the VA territory.
In our study, 19 (67.9%) patients with acute medulla infarction had unilateral VA enhancement on 3D BB contrast-enhanced MRI. Of these, 18 had ipsilateral medulla infarctions. In particular, all type 1 patients (ipsilateral CE+no visualization on MRA) had medulla infarction. The medulla oblongata is mainly vascularized by the VA, anterior spinal artery, lateral spinal artery, and posterior inferior cerebellar artery (PICA), depending on its level. The PICA mostly originates from the VA intracranially, forming perforating arteries on the lateral surface of the brain stem. In other cases, the PICA emerges from the VA extracranially at C1 to provide pial branches for the lateral surface of the brain stem. The lateral spinal artery, also responsible for supplying blood to the posterior part of the medulla, can emerge either from the VA or C1-PICA [17]. In addition, the anterior spinal artery arises from the VA in the proximal part of the lateral spinal artery. Due to the distribution of vessels in the medulla oblongata, short-segment distal VA disease is related to small lateral caudal and/or medium-sized diagonal band-shaped rostral-middle medulla lesions. In addition, long-segment VA disease shows a positive finding of the ventral part of the medulla on DWI [17,18]. At the occlusion site of the VA, 3D BB contrast-enhanced MRI showed strong CE, and MRA showed no visualization of the enhanced VA, which is related to flow stagnation of contrast and slow flow of the distal portion of the occlusion site (Fig. 4A–C) [19]. It has been reported in previous studies that false-negative findings on DWI depend on 2 factors: the size and location of the stroke. When the lesion size is below the spatial resolution power or when the lesion is located in the brainstem, the possibility of the lesion being undetected increases. We also observed false-negative results on initial DWI in 7 patients (25.0%) with symptomatic medulla stroke. After 48 hours, the patients showed delayed positive findings on follow-up images [20]. This indicates that the initial ischemic change due to distal VA occlusion was not sufficient to be detected on early DWI images, but the lesion eventually developed over time and showed positive findings on later DWI images. Patients with delayed positive findings of the medulla on DWI were closely associated with early MR examination after symptom onset. We thought that the delayed positive finding was associated with the progression of ischemia by blood stagnation after occlusion of the distal VA.
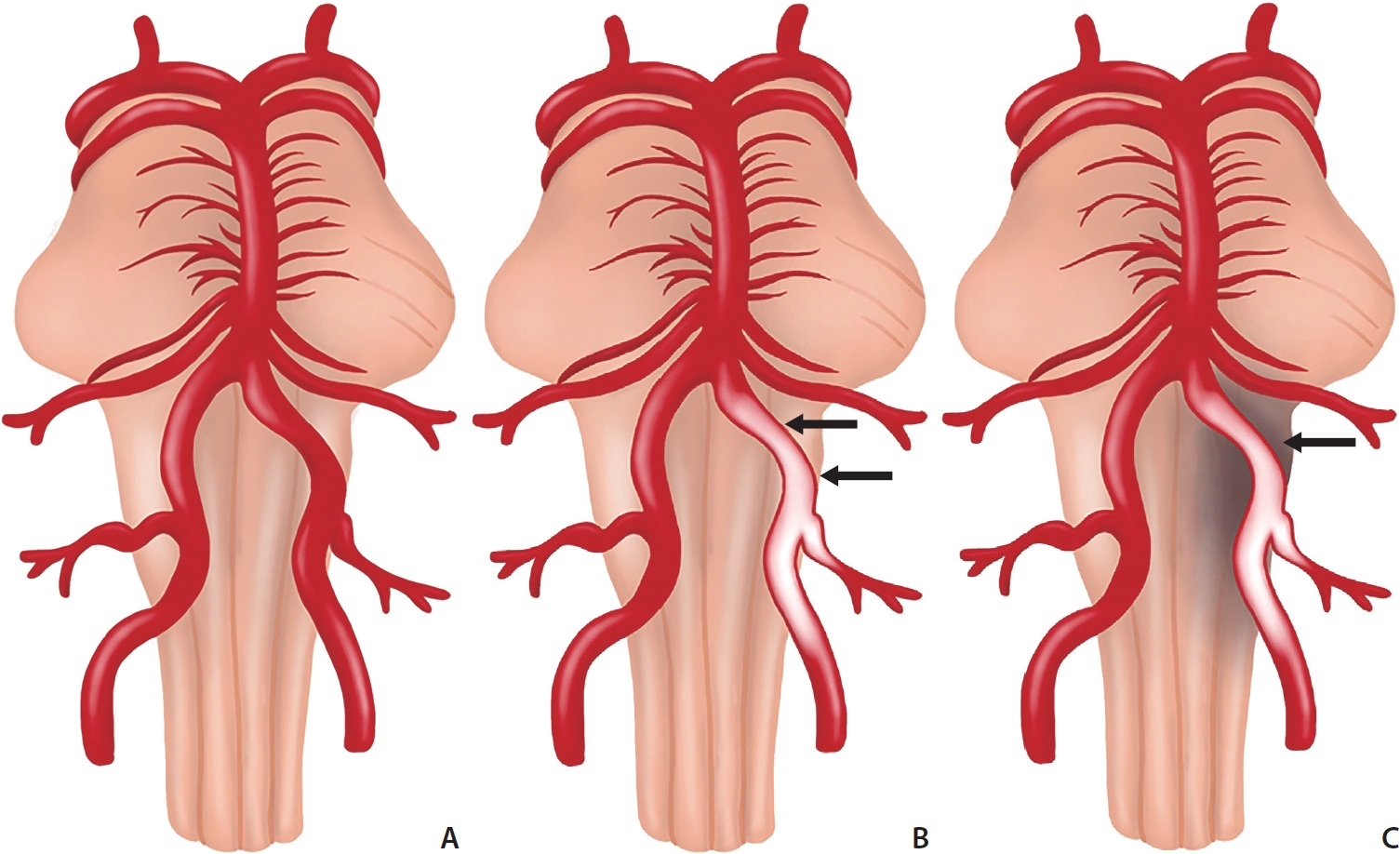
Illustration of acute medulla infarction after occlusion of the distal vertebral artery (VA). (A) Normal VA. (B) Contrast stagnation of the distal VA after acute occlusion of the distal VA (arrows). (C) Acute medulla infarction due to contrast stagnation acute occlusion of the distal VA (arrow). Delayed visualization of acute medulla infarction on diffusion-weighted imaging is associated with ischemic changes after occlusion of the distal VA.
This study has several limitations. First, this was a single-center, retrospective study. Second, because our study focused on acute medulla infarction with positive DWI findings, the sample size was limited to a small number. This may have affected the generalizability of our findings. Therefore, a multicenter prospective study with a larger sample size is necessary. Finally, although the BB-MRI can assess various intravascular lesions, we exclusively described the pattern of BB enhancement in patients with VA occlusion.
CONCLUSION
Unilateral CE of the distal VA on 3D BB contrast-enhanced MRI provides a higher detection rate of acute medulla infarction and is related to the lack of visualization of the VA on MRA. In addition, delayed positive findings of acute medulla infarction on DWI are relatively higher in patients with unilateral CE of the distal VA on 3D BB contrast-enhanced MRI. Early MR examination after symptom onset with acute medullar infarction was associated with initial negative findings and delayed positive findings on DWI. With 3D BB contrast-enhanced MRI, it will be possible to overcome the limitation of delayed DWI by identifying occlusive lesions and treating them in an earlier stage of medulla infarction. To further evaluate the efficacy of 3D BB contrast-enhanced MRI in diagnosing acute medulla infarction, future studies with larger sample sizes and broader ranges of stroke etiology should be followed.
Notes
Fund
This research was supported by a grant of the Medical data- driven hospital support project through the Korea Health Information Service (KHIS), funded by the Ministry of Health & Welfare, Republic of Korea. This paper was also supported by Fund of Biomedical Research Institute, Jeonbuk National University Hospital.
Ethics Statement
All procedures performed in the studies involving human participants were in accordance with the ethical standards of the institutional research committee of Jeonbuk National University Hospital (approval no. JUN 2019- 10-041) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The requirement for patient informed consent was waived for review of patient records and images. We anonymize the patient information that may identify the patient in the figure legends.
Conflicts of Interest
The authors have no conflicts to disclose.
Author Contributions
Concept and design: HSK. Analysis and interpretation: SMC, SYP, and SBH. Data collection: SMC, SYP, and SBH. Writing the article: SMC, SYP, and SBH. Critical revision of the article: HSK. Final approval of the article: HSK. Obtained funding: HSK. Overall responsibility: HSK.