A Case of Coincidental Free Floating Thrombus in the Vertebral Artery in a Patient Presenting with an Anterior Circulation Stroke and Literature Review
Article information

Abstract
Free-floating thrombus (FFT) is a rare condition with unknown etiology as described by many case reports presented in previous literature. The patients usually present symptomatically while the other few patients remain asymptomatic and are usually discovered incidentally on computed tomography angiography (CTA). Most of the cases reported in the literature are of FFT in the internal carotid artery. We present a 59-year-old female as a case of FFT in the vertebral artery which was coincidently discovered on CTA in a patient initially presenting with an anterior circulation stroke. This case highlights the importance of early contrast-based vascular imaging in patients presenting with large vessel strokes that are cardioembolic in nature and the unique utilization of a direct aspiration first pass technique (ADAPT) for revascularization. Included herein an extensive review of the literature about the decision making in patients with FFT and a devised proposed practical approach to this entity.
INTRODUCTION
Free-floating thrombus (FFT) is a rare condition and has been infrequently reported in the literature. The first-ever FFT was reported with postmortem in 1905 [1]. The exact etiopathogenesis of FFT remains unknown, although detached atherosclerotic plaque and hypercoagulable states could be considered as the likely causes [2]. Many case-reports have reported the occurrence of FFT in the carotid artery, mostly the internal carotid artery (ICA). Such patients usually present with a neurological deficit as a consequence of completed stroke with fixed deficits, stroke-in-evolution, or transient ischemic attacks (TIAs) [3]. A few asymptomatic cases have also been reported. The diagnosis of an acute ischemic stroke is done initially with the help of plain computed tomography (CT) and magnetic resonance imaging (MRI). This is followed by CT angiography (CTA) for the confirmation of large vessel occlusion [4]. FFT on CTA is seen as an intra-luminal filling defect and can easily be differentiated from an atherosclerotic plaque [5]. Hence, it is the preferred diagnostic choice in FFT. The available therapeutic management options for such cases are either interventional or medical therapy [6]. A consensus on the optimal management strategy for FFT is not yet established [7]. Bhatti et al. [8] reported that the majority of cases (68%) of FFT underwent surgical management and 30% had medical management with main anticoagulants and antiplatelet therapy. The 30-day postoperative-management outcomes were almost the same in both types of intervention.
We describe a case in which a FFT was discovered coincidently in the vertebral artery in a patient presenting with an anterior circulation stroke. We aim to discuss the importance of early vascular imaging for stroke patients and our acute interventional strategy here. In addition, we conducted an extensive review of the literature about the decision making in patients with FFT and devised a proposed practical approach to this entity.
CASE REPORT
Patient information & diagnostic findings
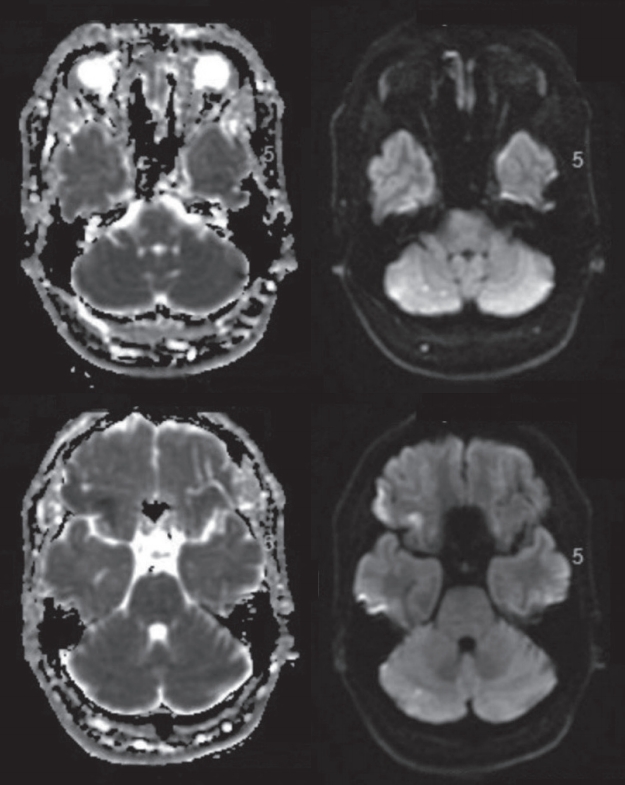
A 59-year-old right-handed Caucasian lady, known to have migraine with aura and type-2 diabetes mellitus presented to our emergency department center with dysarthria, left upper motor neuron facial weakness and left-sided hemiparesis affecting the upper limb more than the lower limb. The patient presented with signs of a right middle cerebral artery (MCA) stroke with an National Institute of Health Stroke Scale (NIHSS) of 10 and unfortunately was out of the window period for intravenous thrombolysis as it was a wake-up stroke and last seen well (LSW) was unknown. A MRI of the brain was obtained on an urgent basis which showed an established infarction in the anterior third of the right MCA territory secondary to the occlusion of the superior M2 branch of the right MCA (Fig. 1).

Magnetic resonance imaging brain showing the sizable right middle cerebral artery (MCA) territory ischemic stroke on FLAIR imaging (upper panel). The magnetic resonance angiography shows the occlusion of the superior branch of the right MCA (lower panel).
Upon further workup, CTA showed a filling defect in the right V4 segment of the right vertebral artery which was suspected of being a dissection or a FFT, with normal flow in the left vertebral artery and the basilar artery and its distal branches (Fig. 2).
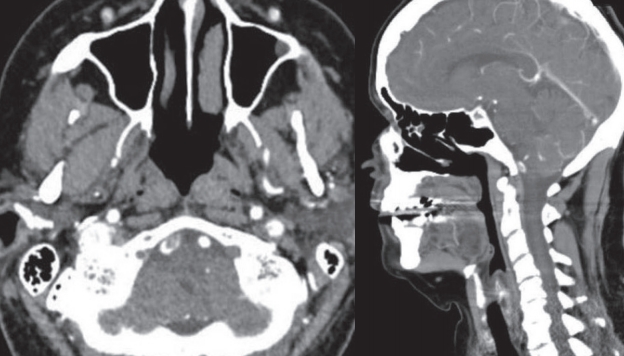
Computed tomography angiography with axial and sagittal demonstration of the free-floating thrombus in the right vertebral artery at the junction of the V3-4 segment. R, right; L, left.
The attending neurologist in the referring hospital discussed the case with our neurovascular on-call team and the patient was then transferred urgently to our hospital for emergent endovascular therapy (EVT).
Intervention
The patient was transferred to King Fahad hospital of the university the same night. An urgent angiogram was performed through a 5-F femoral sheath and a diagnostic catheter, under local anesthesia. The left ICA injection showed a normal flow into the MCA territory as well as the anterior cerebral artery (ACA) territory, with no cross flow to the right hemisphere. The right ICA injection showed the previously mentioned occlusion of the superior M2 branch with deficient collaterals to central MCA core territory. The left vertebral injection showed normal flow in its intracranial segment with no reflux into the right vertebral artery with normal flow into the basilar artery and its distal branches (Fig. 3A). The right vertebral artery was accessed just at its origin and a slow injection of contrast was administered in fear of dislodging any parts of the suspected thrombus. This injection confirmed the presence of the FFT in the V4 segment of the right vertebral artery with non-visualization of the right posterior-inferior cerebellar artery (PICA) or the distal flow into the basilar artery despite minimal filling of the contrast around the clot (Fig. 3B).

Diagnostic and interventional angiogram. (A) Left vertebral angiographic run showing no cross flow into the right vertebral artery. (B) The right vertebral angiographic run showing the filling defect of the free-floating thrombus (FFT) with minimal contrast flow into the distal vertebral artery. (C) The aspirated fragments of the FFT. (D) Right vertebral angiographic run post contact aspiration showing no flow limitation in the vertebral artery with mild stenosis at the V3-4 junction with sluggish flow in the right posterior-inferior cerebellar artery.
Using an exchange wire, The vertebral catheter was exchanged into a 5-F intermediate catheter (Sofia; Microvention, Aliso Viejo, CA, USA). The intermediate catheter, under road map guidance; was advanced with limited wire excursion into the area of the clot. This was followed by manual aspiration that yielded a multiple clot fragments (Fig. 3C). Post aspiration angiogram showed complete revascularization of the right vertebral artery with a slight delay in the right PICA with mild stenosis in the V3-4 junction (Fig. 3D). The patient tolerated the procedure well and remained stable neurologically.
Outcome and follow-up
Immediately after the compilation of the procedure, the patient was transferred uneventfully back to her referring hospital. The MRI obtained 24-hours post thrombectomy showed no new strokes in the posterior circulation territory (Fig. 4). Her stroke workup revealed the significant finding of a left atrial appendage with a thrombus which was discovered through transesophageal echocardiogram (TEE). In addition, she was found to have paroxysmal atrial fibrillation (AF). Given the presence of these 2 risk factors for cardioembolic strokes, the patient was started on anticoagulation in the form of vitamin K antagonist (VKA) warfarin for secondary stroke prevention. A follow-up echocardiogram and TEE were to be done in 3 months to assess the status of the left atrial appendage thrombus but unfortunately, the patient failed to follow up.
Post thrombectomy diffusion weighted magnetic resonance imaging showing no ischemic event in the posterior circulation territory.
DISCUSSION
FFT has been reported in the literature in both the cervical carotid arteries followed by the vertebral arteries with almost all of them presenting symptomatically [8]. These were also termed intraluminal thrombus (ILT), intraluminal clot and were referred to as the doughnut sign [9,10]. Studies based on catheter angiography reported a prevalence of FFT ranging from 0.4% to 1.5% in patients with stroke or TIAs and with the recent utilization of CTA in those patients presenting acutely the prevalence has gone up to almost 3.2% [9-12].
In a recently published study, Singh et al. [12] demonstrated that the most common location of FFT was extracranial ICA at 65.6% followed by extracranial vertebral artery at 11.2%. Intracranial FFT was seen collectively in 18.0% of patients. The intracranial ICA and the basilar artery were each affected in 6.6 % of patients followed by the vertebral artery affected in 3.3% of patients.
The most common cause associated with FFT is atherosclerotic disease of the affected vessel with either complicated plaque (ulcerated or fissured) with or without stenosis. Other possible associations include arterial dissections, cardioemoblic events, and hypercoagulable states [12].
There still remains a debate about the ideal method of treating these patients whether it be medical treatment with the different types of antithrombotics versus EVT such as stenting, stent retrievers and/or a direct aspiration first pass technique (ADAPT) [8,13].
A retrospective study by Gülcü et al. [14] emphasized the use of medical management for resolution of FFT with successful post-management outcome [13]. This can be supported as an option in asymptomatic or stable patients with silent infarcts. In addition, this approach seems to be favored in the presence of non-flow limiting stenosis or dissection with the rapid resolution of the thrombus on serial imaging in the first 2 to 3 weeks of the event.
When managing patients with carotid artery dissection or those with a significant/complicated atherosclerotic plaque, there is a tendency to favor surgical thromboendarterectomy. This is thought to minimize vessel manipulation and allows for placing intimal tacking sutures which can prevent flap progression which reduces the risk of cerebral embolism.
In the recent literature, there is a trend to utilize endovascular therapies for FFT. These can be offered either acutely or in a delayed manner mostly targeting residual stenosis. These options include clot contact aspiration with the ADAPT technique or stenting. ADAPT is a simple, efficient, and safe technique for revascularization of large vessel occlusion in patients with acute ischemic stroke [15]. It was found to have a favorable profile with proximal occlusion and when the culprit for the FFT is deemed inflammatory arteritis [16]. If the artery is found to have a residual stenosis that is flow-limiting, we would advocate for stenting of the offending plaque in an expedited manner. These options lend themselves to debate when the offending vessel is in the anterior circulation. In contrast, the treatment options of posterior circulation vessels affected by FFT are limited to either medical therapy or endovascular means. There is no consensus of the management protocol for FFT. We summarized the existing literature on this entity in Table 1 [3,7,8,12,16-41]. Although it is difficult to establish a consensus on a management approach for FFT, we devised as proposed practical approach to FFT in a decision tree presented in Fig. 5.
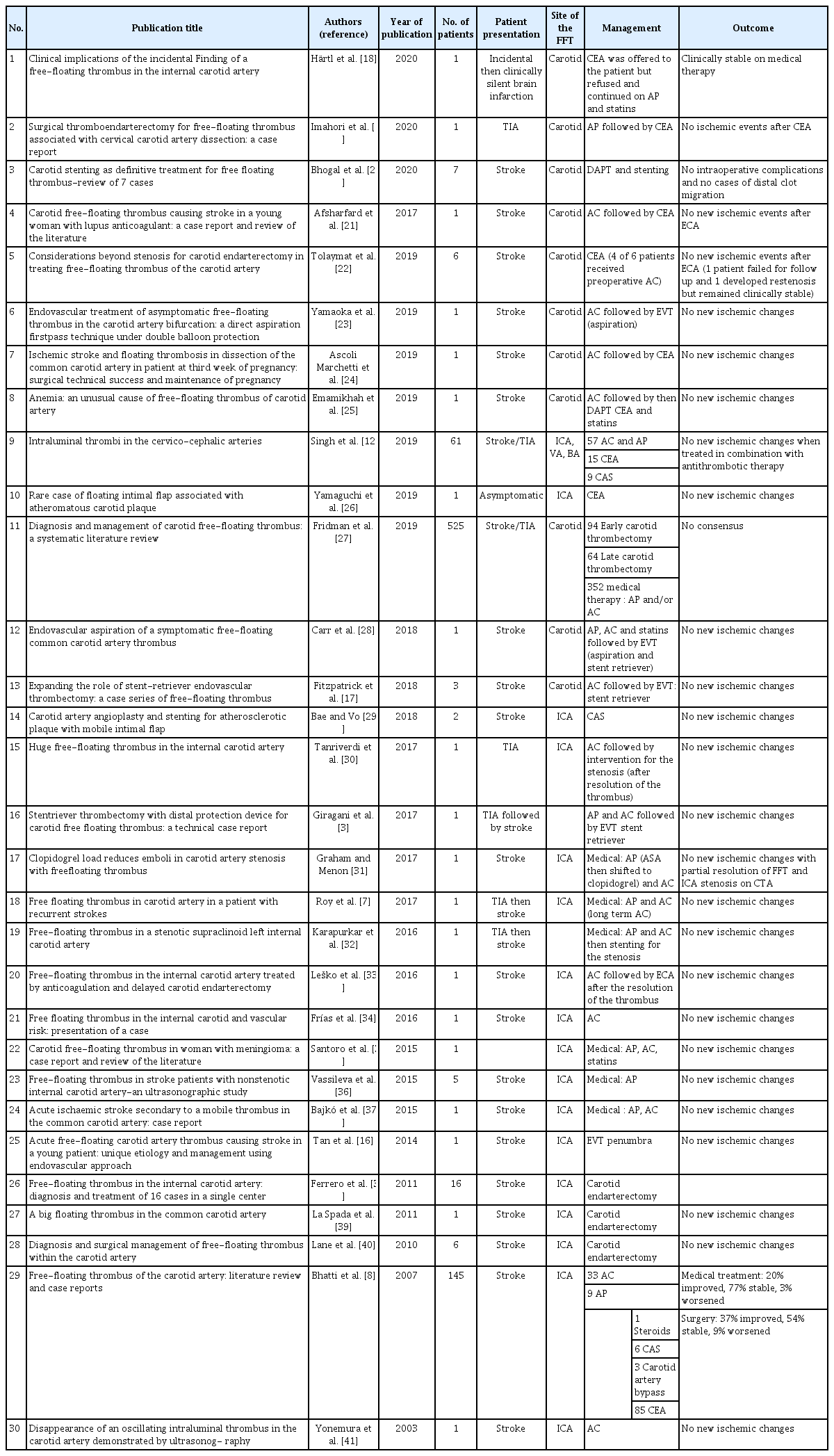
Review of the current literature on FFT
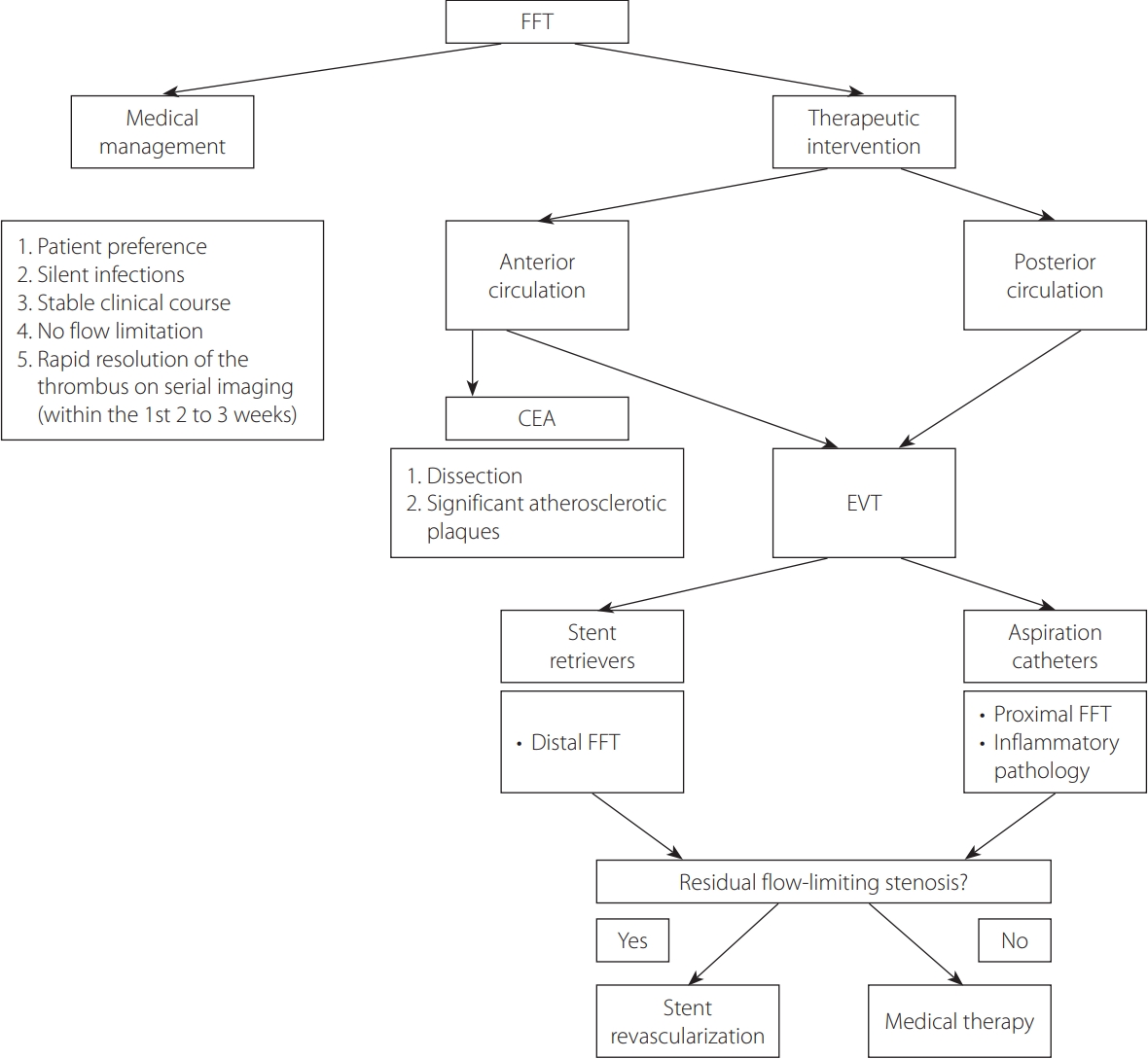
A proposed practical approach to free-floating thrombus (FFT). CEA, carotid endarterectomy; EVT, endovascular therapy.
Our patient had symptoms primarily related to an acute ischemic MCA stroke. She did not manifest any symptoms related to posterior circulation, despite harboring a FFT in the vertebral artery, which was incidentally observed during imaging. This stresses the importance of CTA in detecting FFT especially in asymptomatic cases like ours.
To our knowledge, this represents the first case reported in the English literature of an asymptomatic FFT in the vertebral artery in a patient presenting with an MCA stroke. It is extremely fascinating that the FFT in this patient’s right vertebral artery remained clinically silent, despite the lack of direct filling in the right PICA, which could have rendered her with defects if not a full-blown Wallenberg syndrome.
In our patient, we opted for EVT over medical therapy in fear of the risk of hemorrhagic transformation in the sizable ischemic MCA infarct. To that end we chose ADAPT as our first option of interventional management. From a technical stand point, this technique mitigated any wire or microcatheter manipulation that might have dislodged the clot into the basilar artery, which poses a significant risk of morbidity. We also used an almost wire-less advancement of the intermediate catheter especially beyond the V2-3 junction to avoid the same potential of inadvertent clot manipulation.
This case illustrates the importance of obtaining an early contrast-based vascular imaging in all patients affected with acute ischemic stroke to be able to visualize anterograde and retrograde flow in any given vessel. This would help in stratifying risks and needed interventions accordingly.
In conclusion, this is the first reported case of an asymptomatic FFT in the vertebral artery that was discovered coincidently in a patient presenting with an anterior circulation stroke. It highlights the importance of early acquisition of vascular imaging for all stroke patients and the timely utilization of EVT (ADAPT) as a safe and preferred method of acute revascularization in such cases.
Notes
Fund
None.
Ethics Statement
An informed consent was obtained from the patient for publication of this paper.
Conflicts of Interest
The authors have no conflicts to disclose.
Author Contributions
Concept and design: HAJ and MAA. Analysis and interpretation: HAJ and MAA. Data collection: MAA and YA. Writing the article: MAA and HAJ. Critical revision of the article: HAJ, YA, and FA. Final approval of the article: HAJ, MAA, and FA. Statistical analysis: MAA. Obtained funding: none. Overall responsibility: HAJ.