Hairball-Like Migration of “Onyx Threads” into the Draining Vein during Transarterial Embolization of a Dural Arteriovenous Fistula: A Case Report and Experimental Validation
Article information

Abstract
Transarterial embolization using Onyx is a well-established treatment for dural arteriovenous fistulas (DAVFs). However, complications can arise when Onyx migrates into the venous side, impairing the draining veins. We encountered a case where Onyx, injected through the arterial side, strayed into the jugular vein, forming a hairball-like structure. Our study aimed to investigate the underlying mechanism of this unusual phenomenon. We postulated that Onyx precipitates into thread-like shapes when passing through extremely narrow openings. To test this, we extruded Onyx from a syringe through a 27-gauge needle into a silicone tube with flowing water. By varying the flow speed, we observed the hardening behavior of Onyx. Under slow flow, the extruded Onyx quickly solidified at the needle tip, forming a round mass. Conversely, high-speed flow resulted in Onyx being dispersed as small pieces. We successfully replicated the formation of “Onyx threads” under continuous slow flow conditions, similar to our case. This phenomenon occurs when Onyx unexpectedly migrates to the draining vein through a tiny opening during transarterial embolization for arteriovenous shunt diseases. Early recognition and appropriate measures are necessary to prevent occlusive complications in the draining veins and the pulmonary system.
INTRODUCTION
Transarterial embolization with Onyx (Medtronic) is currently an established method of treatment for dural arteriovenous fistulas (DAVFs) [1,2]. Onyx is cohesive and nonthrombogenic, which allows for better packing of lesions and makes venous occlusion less likely than n-butyl cyanoacrylate. Onyx occasionally passes to the draining vein during the packing of the shunt portions, but the cast usually slowly moves forward and hardens at the entrance of the draining vein side while sticking to the draining vein’s wall. However, we encountered a unique finding of intravenous Onyx migration during transarterial embolization of a transverse sigmoid sinus DAVF. A hairball-like structure suddenly appeared in the jugular vein during Onyx injection. It was removed transvenously and confirmed to be an Onyx thread on pathological examination. This brief report aimed to determine the mechanism underlying this abnormal phenomenon in an experimental simulation.
CLINICAL CASE AND EXPERIMENTAL VALIDATION
A 66-year-old man presenting with pulsatile tinnitus was diagnosed with a right jugular bulb and transverse sigmoid sinus DAVF and was referred to our hospital for endovascular treatment (Fig. 1A, B). Under general anesthesia, 6-Fr long sheaths were inserted into the right femoral artery and vein. A 6-Fr guiding catheter was navigated into the right jugular vein and external carotid artery. First, we performed a transvenous embolization of the fistula in the jugular bulb. A Headway 17 microcatheter (Terumo) was navigated through a shunting pouch around the right anterior condylar confluence. The detachable coils were deployed in a shunting pouch. Then, a transarterial embolization of the right external carotid artery was performed. The feeders of the right ascending pharyngeal, right posterior auricular, and right middle meningeal arteries were embolized using Onyx-18 (Medtronic). Finally, a Scepter balloon catheter 4×7 mm (Terumo) was navigated into the right occipital artery, and Onyx was administered. We inflated a Shouryu balloon catheter 7×7 mm (Kaneka) inside the right transverse sigmoid sinus to avoid Onyx migration into the venous side during injection (Fig. 1C, D). An abnormal thread-like black line connected to the injection site was observed on the digital subtraction angiography monitor during Onyx injection from the Scepter balloon catheter (Terumo). The origin of this thread was proximal to the inflated balloon for sinus protection. It accumulated in the jugular bulb as a hairball-like mass (Fig. 1E, F). The injection was stopped, and the Scepter catheter was removed. The foreign body in the jugular vein was retrieved using a goose-neck snare 10 mm (Medtronic) (Fig. 1G, H), and a black thread-like mass was identified (Fig. 1I). The pathological result of the foreign body was revealed to be Onyx. The transverse sigmoid sinus DAVF was treated with transvenous sinus packing using coils (Fig. 1J–L). Almost all the shunts disappeared, as well as the patient’s tinnitus, immediately after the operation.
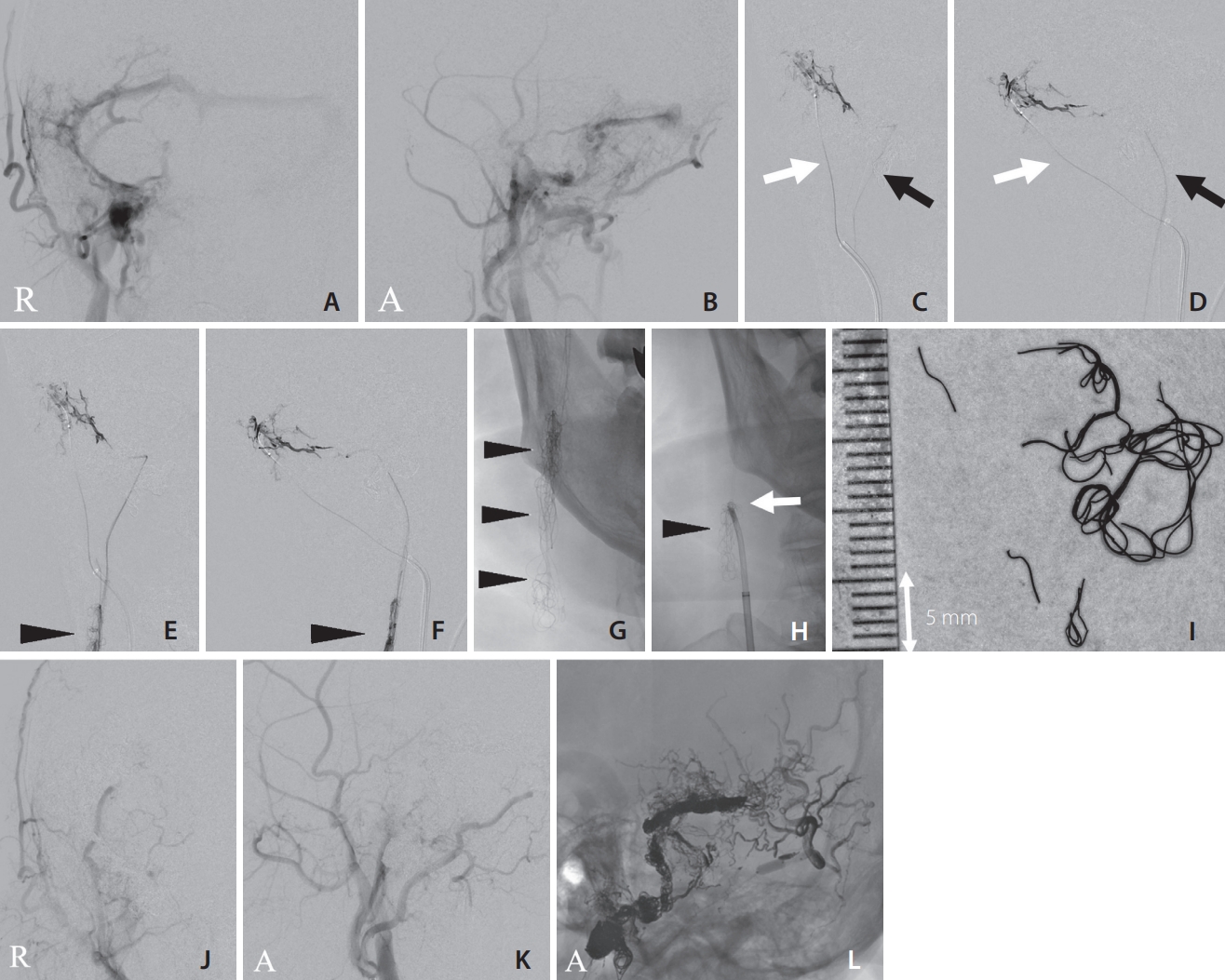
(A) Preoperative angiography. Anterior–posterior view of right external carotid angiography showing the dural arteriovenous fistula (DAVF). (B) Preoperative angiography. Lateral view of right external carotid angiography showing the DAVF. (C, D) Angiography during Onyx injection before migrating into the venous side (C: anterior–posterior view, D: lateral view). The white arrows indicate the Scepter balloon catheter (Terumo) in the right occipital artery. The black arrows indicate the Shouryu balloon catheter (Kaneka) in the transverse sinus. (E, F) Angiography during Onyx injection just after the migration into the venous side (E: anterior-posterior view, F: lateral view). The black arrowheads indicate a hairball-like structure in the right jugular vein. (G) A hairball-like foreign body seen in the jugular vein on fluoroscopic imaging (black arrowheads). (H) The foreign body (black arrowhead) was retrieved by clamping with a goose-neck snare and a 4-Fr diagnostic catheter (white arrow). (I) Photograph of the retrieved foreign body. (J) Postoperative angiography. Anterior–posterior view of the right external carotid angiography. (K) Postoperative angiography. Lateral view of right external carotid angiography showing that shunt reduction was achieved. (L) Onyx cast and coils placed in the transverse sigmoid sinus. R, right side; A, anterior direction.
We planned an experimental model to determine the mechanism underlying this abnormal phenomenon. We hypothesized that Onyx precipitates in a thread-like shape when passing through an extremely narrow hole. Therefore, Onyx was extruded from a syringe using a 27-gauge needle into a silicone tube with flowing water. In this experiment, we changed the flow speed of the water and observed the hardening behavior of Onyx (Fig. 2). The extruded Onyx quickly hardened at the needle tip and formed a round mass under very slow flow. Onyx was blown away as small scattering pieces under high-speed flow. Onyx threads were successfully formed only under the adequate continuous slow flow condition (Supplementary Video 1).
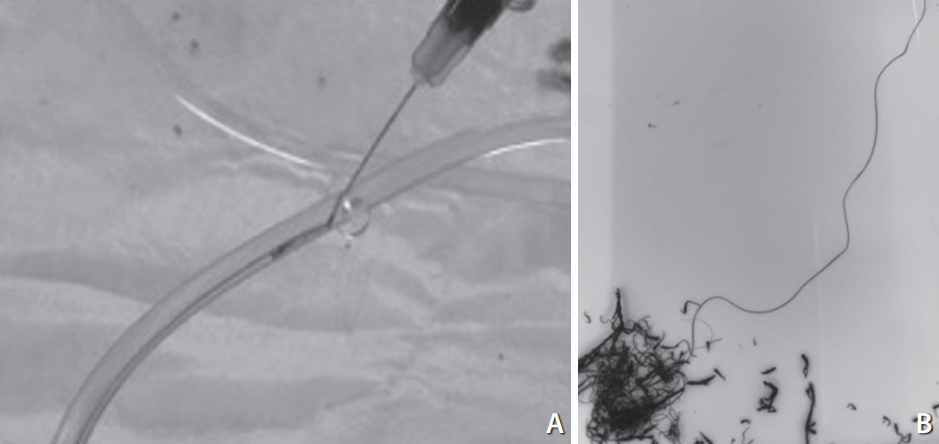
Photograph of the in vitro experiment. (A) Onyx was injected using a 27-gauge needle into water. (B) The Onyx was precipitated in a thread-like manner and accumulated as a hair-ball-like structure.
DISCUSSION
Transarterial Onyx embolization for DAVFs is a safe and effective therapeutic alternative [1,2]. However, migration of Onyx to the venous side through the shunt point impairs normal venous drainage and increases the risk of pulmonary embolism. Wang et al. [3] reported a case of cardiac Onyx migration that required thoracic surgery. They also reported a case of deep cerebral venous occlusion that led to deterioration or death. Therefore, we usually use a large protective balloon in the affected sinus to avoid such venous migration and preserve normal sinus blood flow.
Transarterial balloon-assisted embolization combined with transvenous sinus balloon protection using a transvenous balloon is reportedly a useful adjunctive technique for the treatment of DAVFs [4]. Using this method, greater penetration into the shunting points of Onyx and less migration into the venous side can be expected compared with other conventional methods. However, the shape of the cross-section of the sinus is not round, and many trabeculations exist in the cavity. Therefore, complete balloon attachment to the sinus wall is difficult, and the balloon does not always cover all shunt points for DAVF with multiple shunt points, similar to our case. We used a relatively short balloon because a long, super-compliant balloon (e.g., 80 mm in length) is not approved for use in Japan. Therefore, migration of Onyx to the venous side occurred.
Onyx penetrating the venous side usually forms a claylike mass at the exit of the shunt point. However, in this case, Onyx hardened into a thread-like shape and continuously jetted out without breaking. If this mass had migrated into the pulmonary artery, a serious complication would have occurred; however, the Onyx threads remained in the jugular vein in 1 lump, forming a hairball. Therefore, it was easily retrieved using a goose-neck snare.
Our study demonstrated that the extruded Onyx quickly hardened at the needle tip and formed a round mass under very slow flow, whereas Onyx was blown away as small scattering pieces under high-speed flow. Onyx threads were successfully formed only under an adequate continuous slow flow condition, similar to our case. These results indicate that transarterially injected Onyx penetrated through a tiny channel connected to the sinus wall and precipitated continuously by applying constant pressure in a less pulsatile and stable venous flow in the sinus. The size of the shunt area varies, as previously reported, with cases ranging from micro-pinholes to >3 mm in diameter [5], but accidents during the transarterial injection of Onyx are caused by tiny channels in the perisinus network directly connected to the sinus. Onyx threads may be overlooked because they are thin and sway, and the operator usually watches only the shunt point. Physicians should be aware of this complication when similar intraoperative phenomena are observed.
CONCLUSION
In conclusion, “Onyx threads” can be formed by injecting Onyx from a small hole under an adequately slow continuous flow condition. This phenomenon occurs when Onyx unexpectedly migrates to the draining vein side through a tiny hole during transarterial embolization for arteriovenous shunt diseases. Therefore, early recognition and measures with complete sinus balloon protection are mandatory to avoid occlusive complications in the draining vein and pulmonary system.
SUPPLEMENTARY MATERIALS
Supplementary materials related to this article can be found online at https://doi.org/10.5469/neuroint.2023.00185.
Supplementary Video 1.
Notes
Fund
None.
Ethics Statement
This study waived approval of the Institutional Review Board (IRB), and IRB approval for case reports is not required at our institution. We obtained individual written informed consents for the procedure and for publication.
Conflicts of Interest
The authors have no conflicts to disclose.
Author Contributions
Concept and design: TI, TO, MY, NM, and SM. Analysis and interpretation: TI, TO, MY, NM, and SM. Data collection: TI, TO, MY, NM, and SM. Writing the article: TI, TO, MY, NM, and SM. Critical revision of the article: TI, TO, MY, NM, and SM. Final approval of the article: TI, TO, MY, NM, and SM. Statistical analysis: TI, TO, MY, NM, and SM. Overall responsibility: TI, TO, MY, NM, and SM.