Endovascular treatment (EVT) has become an established procedure for treating intracranial aneurysms. Over the past 20 years, reports of this technique and its outcomes have been published by endovascular specialists [1,-7]. In 2002, the results of the International Subarachnoid Aneurysm Trial (ISAT) demonstrated the clinical superiority of EVT over standard surgical treatment for ruptured intracranial aneurysm [7]. Some published articles have examined the eff icacy of detachable coils for stabilizing occlusions and providing protection against the growth or regrowth of aneurysms and consequent bleeding [1,-3]. The widespread use of detachable coils for endovascular coil embolization of intracranial cerebral aneurysms has made EVT mainstay of aneurysm treatment. Nonetheless, there have been few data in the outcomes of younger patients' EVT for intracranial cerebral aneurysms [2,, 8,-13]. The purpose of this study was to provide an overview of the clinical and radiologic outcomes of endovascular coil embolization for cerebral aneurysm in patients aged 40 years and younger.
MATERIALS AND METHODS
Patient Demographics
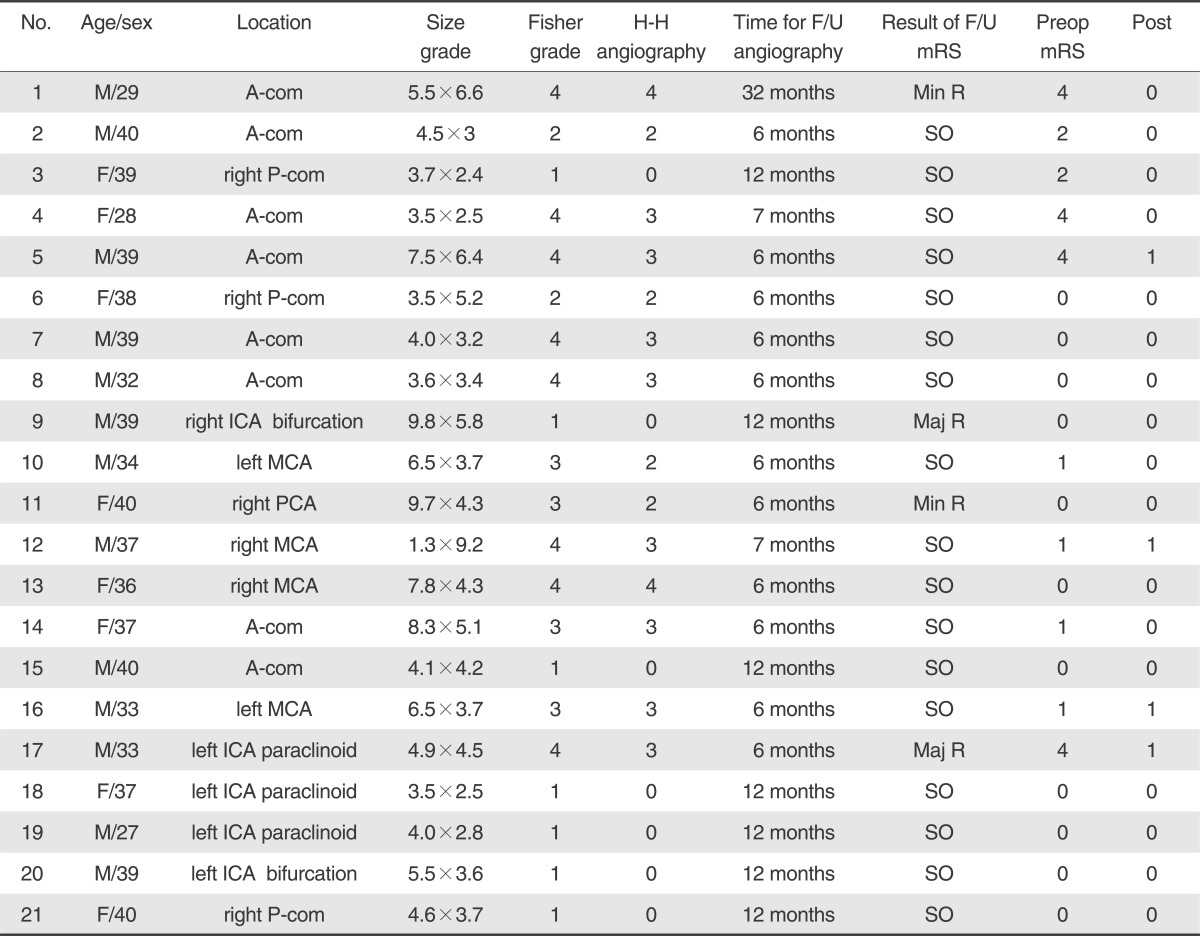
Between January 2008 and June 2011, 294 cerebral aneurysms in 249 patients were treated by two neurointerventionalist (one neurosurgeon and one neuroradiologist) using endovascular coil embolization. Dissecting, fusiform, infectious or traumatic aneurysms were excluded. Of these, 218 aneurysms in 200 patients with follow-up angiography at least six months were included in this study. Twenty-one aneurysms (14 ruptured [66.6%] and seven unruptured [33.3%]) occurred in 21 patients aged 40 years and younger (mean age: 33.5 years; range: 27-40 years). Of these, 13 patients were men, and eight were women. The mean angiography follow-up period was 9.3 months ┬▒ 2.69 in the younger group. A total of 197 aneurysms (96 ruptured [48.7%] and 101 unruptured [51.3%]) occurred in 179 patients older than 40 years (mean age: 61.8 years; range: 41-84 years). Of these, 70 patients were men, and 127 were women. The mean angiography follow-up period was 9.2 months ┬▒ 2.54 in the older group.
Procedure
We performed coil embolizations for all cerebral aneurysm through the common femoral artery under general anesthesia. In case of aneurysms with wide necks or unfavorable shapes, we used the methods of double catheter, balloon or stent-assisted coil embolization. Patients with unruptured aneurysms electively underwent endovascular coil embolization, and patients with ruptured aneurysms underwent within 24 hours. After the completion of coil embolization, we divided the angiographic findings into three classes using the modified Raymond scale: complete occlusion, neck remnant, and residual aneurysm [12]. An aneurysm was classified as completely occluded when there was no contrast filling within the aneurysm. Aneurysms were classified as neck remnant when there was some contrast near the aneurysm neck. A residual aneurysm was determined when some contrast was seen in the aneurysm neck and dome.
Angiographic and Clinical Follow-up
We checked the follow-up cerebral angiography to disclose recanalization at least six months after treatment. We classif ied minor recanalization as minimal coil compaction at the aneurysm neck, and major recanalization as contrast filling within the dome of the aneurysm or significant coil compaction. We checked the clinical outcomes before the procedure and at follow-up angiography using the modified Rankin scale scores (mRS). Clinical outcomes were reviewed from clinical charts.
Statistical Analysis
All of data were analysed using Statistical Package for Social Sciences (SPSS version, 19.0, SPSS Inc., USA). Chi-square test was used to compare general characteristic frequencies. Fisher's exact test was used to compare aneurysm location frequencies and recanalization rate between age group. Mann-Whitney U test was used to evaluate clinical outcome score between age group. Significance level was set as 0.05.
RESULTS
Aneurysm Location
Among 21 aneurysms in young age group, there were 20 anterior circulation aneurysms and one posterior circulation aneurysms. The anterior communicating artery (8 aneurysms, 38.0%), middle cerebral artery (MCA) (4 aneurysms, 19.0%) and paraclinoid internal carotid artery (ICA) (3 aneurysms, 14.3%), posterior communicating artery (3 aneurysms, 14.3%) were frequent sites. Total of 197 aneurysms in other group, there were 189 anterior circulation aneurysms and 8 posterior circulation aneurysms. Almost aneurysm locations were not different between two groups, however the difference in the ICA bifurcation aneurysm rate was statistically significant between the two groups (Table 3). The distribution of all groups' aneurysm location was similar to a previous study [7].
Immediate Angiographic Findings
All immediate angiographic findings were evaluated and classified by an independent investigator. The initial angiographic outcomes for the aneurysms in patients aged 40 years and younger were complete occlusion in 18 (85.7%) and neck remnant in three (14.3%). There was no residual aneurysm. The initial angiographic outcomes for aneurysms in patients older than 40 years were complete occlusion in 179 (90.8%), neck remnant in 17 (8.6%), and residual aneurysm in one (0.5%). The differences between the two groups were not statistically significant.
Follow-up Angiographic Findings and Retreatments
Angiographic follow-up involved conventional angiography with DSA. All angiographic follow-up were evaluated and classif ied by an independent neuroradiologist. Recanalizations were noted in four aneurysms (19.0%) in patients aged 40 years and younger. Two (9.5%) were minor recanalizations of ruptured aneurysms and two (9.5%) were major recanalizations, one in a ruptured aneurysm and the other in an unruptured aneurysm. The major recanalization was located at the bifurcation of the internal carotid artery in the unruptured aneurysm and at the internal carotid artery of the paraclinoid segment in the ruptured aneurysm. Additional coil embolizations were performed in these two cases. Recanalizations were noted in 41 aneurysms (21.1%) for patients older than 40 years: 35 (17.7%) were minor recanalizations and six (3.0%) were major recanalizations. Of these minor recanalizations, 17 were ruptured aneurysms and 18 were unruptured aneurysms. All major recanalizations were in ruptured aneurysms: two located at the posterior communicating artery, three at the MCA, one at the basilar tip and one at the superior cerebellar artery. Additional coil embolizations were performed successfully with no complications in these six cases of major recanalization. The difference in recanalization rate between the younger and older groups was not statistically significant. Also, the difference in recanalization between ruptured and unruptured aneurysms was not statistically significant (Table 4).
Clinical Outcomes
No bleeding or rebleeding of cerebral aneurysms was detected during follow-up angiography. Procedure-related complications occurred in two (9.5%) out of 21 patients including one non-symptomatic angiographic thromboembolic event (4.7%) and one non-symptomatic internal carotid dissection (4.7%) in a patient under 40 years. There was no procedure-related major stroke or deaths. The preoperative mean mRS was 1.14, and the postoperative mean mRS was 0.19 at the time of follow-up angiographies of patients aged 40 years and younger. The preoperative mean mRS was 1.30, and the postoperative mean mRS was 0.30 at the follow-up angiographies of patients older than 40 years. The difference between groups was not statistically significant (preoperative mRS, p-value: 0.837; postoperative mRS, p-value: 0.934) (Table 5).
DISCUSSION
In our study, approximately 9.6% (21 of 218) of aneurysms in patients aged 40 years and younger were treated with coil embolization. 12.7% (14 of 110) of the ruptured aneurysms in patients aged 40 years and younger were treated by coil embolization.
A male dominance in young age group was noted compared with other group (Table 1), and this difference was statistically significant. The male dominance among patients with SAH has been described in childhood and adolescence, however the female ascendancy is described in adult group of patients [14,, 15].
In aspect aneurysm location, ICA bifurcation aneurysm rate was statistically higher in young patients than in old patients (Table 3). Previous authors have noted that a vast majority of ruptured aneurysms in children and adolescents occur in the anterior circulation, especially in the ICA [16,, 17]. The ICA has a blood flow much greater than the anterior communicating artery and MCA. Such flow may exert intense hemodynamic stress on the arterial walls and thus, result in the formation of an aneurysm and rupture [16,-18].
A previous study found that age had no significant impact on the recanalization of cerebral aneurysm [12], but many other factors influence recanalization, including aneurysmal height and neck width, aneurysm location, and ruptured aneurysm [9,,12,, 16,-19]. In our study, the difference in recanalization between ruptured and unruptured aneurysms in each group was not statistically significant (Table 4). Previous studies reported wide variations in aneurysm recanalization rates ranging from zero to 42% [9,, 12,, 20,-25]. Our study showed a 19% recanalization rate among patients aged 40 years and younger. When a major recanalization was found, we checked the cerebral angiography regularly. The primary treatment of choice for major recanalization in our hospital is recoiling. In present study, there were no statistically significant differences in recanalization between the two groups of patients (those aged 40 years and younger and those older than 40 years). Although our study showed a modest recanalization rate (19%), there were no cases of bleeding or death during our follow-up.
Our study showed favorable clinical results of coil embolization for intracranial aneurysms with little procedure-related morbidity [9.5% (two out of 21)] and no procedure-related deaths. Patients aged 40 years and younger had favorable outcomes on the preoperative and postoperative mRS, but they were not statistically significant (preoperative mRS: 1.14; postoperative mRS: 0.19).
Although the rate of ruptured aneurysms in young patients was higher than other group (14/21 [Ōēż40 years old, 66.6%] versus 93/197 [>40 years old, 47.2%]), difference of recanalization rate and clinical outcomes was not statistically significant. Although there was no definite recommendation of treatment for young patients with aneurysm, in general surgical clipping is preferred in young patients because of its durability and minimal surgical risk. Patients treated with endovascular therapy in the present study had good early clinical outcome with no perioperative mortality. Even though it has been a short term follow-up, there were no fatal procedural complications with endovascular treatment and complete aneurysm occlusion was noted in almost cases. Our results suggest that endovascular therapy can be a viable option in young patients with aneurysm as it seems to provide excellent clinical outcomes with high aneurysm occlusion rates and tolerable recanalization rates. But regular radiological and clinical follow up would be necessary, considering the remaining years of the patients.
Our study has some limitations. The first is the lack of an analysis of the relationship between recanalization and aneurysm location. As aneurysms at the bifurcation have higher recanalization rates than aneurysms at other locations, aneurysm location and hemodynamic changes could be related to recanalization rates [26]. Because of the small number of patients in our study, we could not analyze the significance of aneurysm location. The second limitation is that we did not evaluate the coil packing density after aneurysm coil embolization. Coil packing density is an important factor for recanalization but accurate calculation of coil packing density is very difficult because of the irregular aneurysm shape and 3D configuration. The third limitation is the short follow-up period of cerebral angiography. In our study, the mean angiographic follow-up was 9.3 months. So, long-term cerebral angiography follow-up is required for cerebral aneurysm patients undergoing coil embolization and we need to establish the relation between cerebral angiography follow-up and recanalization after complete coiling of an aneurysm.
In conclusion, the younger patients had clinically favorable outcomes with tolerable angiographic follow up results. Because they have a longer life expectancy, patients aged 40 years and younger treated by endovascular coil embolization should undergo more regular and long-term imaging follow-up.