INTRODUCTION
Extracranial atherosclerosis (ECAS) is observed in about 10ŌĆō20% of stroke patients and is not a rare cause of acute ischemic stroke [1,2]. Retrospective single-arm studies have shown that acute ischemic stroke patients undergoing emergent endovascular treatment (EVT) for acute extracranial internal carotid artery (ICA) occlusion show high recanalization rates and early neurologic improvement [3-5]. In addition, several studies have demonstrated that patients with extracranial occlusion combined with intracranial artery tandem occlusion have better outcomes after EVT [6-8]. Mechanical thrombectomy-based EVT is now considered a reasonable treatment especially for intracranial large artery occlusions [9]. However, symptomatic intracranial hemorrhage (ICH) is observed in about 30ŌĆō40% patients with acute large-artery occlusion after EVT [10,11], and it is thus considered a significant contributing factor for poor functional outcomes.
Carotid artery stenting is an EVT option for patients with extracranial carotid stenosis. Cases of extracranial stenting (ES) for ECAS-related occlusion in hyperacute stroke are increasing presently; however, the relationship between ES and the prevalence of post-procedural hemorrhagic transformation (HT) remains unclear. Therefore, we investigated the association between ES and the prevalence of post-procedural HT and assessed the effect of ES on clinical outcomes in patients with hyperacute stroke.
MATERIALS AND METHODS
Study population and inclusion criteria
We retrospectively analyzed patients in the Acute Stroke due to Intracranial Atherosclerotic occlusion and Neurointervention-Korean Retrospective (ASIAN-KR) registry. This registry collected data on patients (aged Ōēź18 years) who underwent EVT for cervicocerebral artery occlusion causing ischemic stroke at three comprehensive stroke centers in Korea between January 2011 and February 2016 [12]. Inclusion criteria were as follows: 1) onset-to-puncture time within 24 hours; 2) underlying etiology was proven as ECAS; or 3) patients underwent EVT for extracranial artery steno-occlusive disease.
All clinical data were de-identified and allocated study identification numbers. The protocol of data collection was approved by the Institutional Review Board of each hospital and was implemented in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments.
Evaluation methods
Premorbid and 3-month modified Rankin Scale (mRS) scores, National Institutes of Health Stroke Scale (NIHSS) scores, conventional vascular risk factors, and laboratory findings on admission were collected. A 3-month mRS score of 0 to 2 or no change compared with the premorbid mRS score was defined as a good outcome, and a 3-month mRS score of 3 to 6 or an increase compared with the premorbid mRS score was classified as a poor outcome.
The location of the initial occlusion site was determined using baseline computed tomography (CT) angiography, magnetic resonance angiography, or digital subtraction angiography. Stenotic degree of extracranial artery associated with hyperacute stroke was assessed based on the North American Symptomatic Carotid Endarterectomy Trial criteria [13]. Alberta Stroke Program Early CT Scores (ASPECTS) were determined using non-contrast CT in the anterior-circulation territory in patients with hyperacute stroke. Final reperfusion was evaluated using the modified thrombolysis in cerebral infarction (mTICI) scale [14], and mTICI grades 2b or 3 were defined as successful reperfusion. Post-procedural ICH was graded based on the criteria defined by the European Cooperative Acute Stroke Study, and was defined as presence of any grade of ICH for the current study [15]. Subarachnoid hemorrhage was classified according to the modified Fisher scale [16].
Endovascular procedures
Endovascular devices were selected at the discretion of neurointerventionists based on consensus within each stroke team. Contact aspiration and stent retrieval were routinely used as a frontline method. Contact aspiration is a method of a forced arterial suction thrombectomy, which uses the Penumbra system (Penumbra Inc., Alameda, CA, USA). Stent retrieval is a method of clot removal by capturing and removing the thrombus with a stent retriever, such as the Solitaire AB/FR (Medtronic, Irvine, CA, USA) or Trevo (Stryker, Kalamazoo, MI, USA). Balloon guide catheters, adjuvant local lytic infusion, intracranial or extracranial angioplasty, and/or stenting were implemented as needed.
Statistical analysis
Data are expressed as mean┬▒standard deviations, median (interquartile ranges), or numbers (percentages). Comparative analyses of clinical characteristics and treatment outcomes were performed between the ES and non-ES (NES) groups. Differences between the groups were analyzed using Žć2 tests for categorical variables, the Mann-Whitney U-test for ordinal variables, or t-tests for continuous variables. To evaluate the relation between ES and the prevalence of post-procedural ICH or further clinical outcomes, we performed multivariate logistic regression analyses with major confounders. A P of <0.05 was considered significant. Statistical analyses were performed using the SPSS statistical package (version 25.0, IBM SPSS, Armonk, NY, USA).
RESULTS
Baseline characteristics
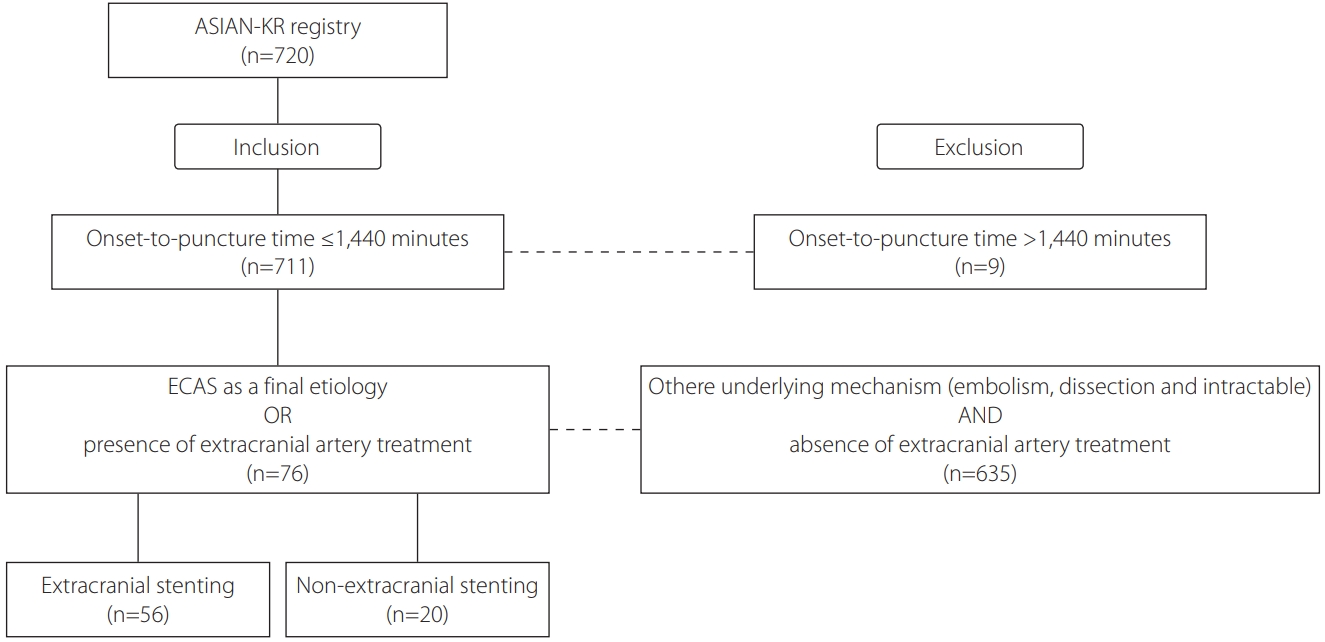
Among the 720 registered patients, 76 patients were eligible based on the inclusion criteria (Fig. 1). Baseline characteristics of patients are summarized in Table 1. Among the 76 eligible patients, 56 patients underwent ES, and 20 patients did not undergo any extracranial treatment or underwent other extracranial treatments without stenting (such as balloon-angioplasty and contract aspiration). Atrial fibrillation was more prevalent in the NES group than in the ES group (35.0% vs. 7.1%, P=0.002); however, other variables including laboratory data; percentages of hypertension, diabetes mellitus, dyslipidemia, or smoker; NIHSS or ASPECTS score on admission; or systolic or diastolic blood pressure did not differ between the two groups.
Treatment methods and outcomes associated with ES
Comparative analyses of treatment methods and outcomes between these two groups are summarized in Table 2. Overall procedure time or treatment methods, except for the ES, were not different between the two groups. The rates of successful reperfusion were similar in these two groups, regardless of ES (80.0% vs. 85.7%, P=0.547). Functional outcomes, based on the mRS score, did not differ between the ES and NES groups. However, the prevalence of post-procedural cerebral hemorrhage after emergent extracranial EVT was associated with ES (odds ratio [OR], 7.807; 95% confidence interval [CI], 1.213 to 50.248; P=0.031) (Table 3). Notably, multivariate analyses with potential major confounders in a logistic regression model revealed that the presence of ES was the only independent predictor for the prevalence of hemorrhage after emergent extracranial EVT (OR, 7.807; 95% CI, 1.213 to 50.248; P=0.031). Good outcomes at 3 months were more commonly observed in patients without than with any post-procedural cerebral hemorrhage (68.0% vs. 42.3%, P=0.031).
As observed in Table 4, the association between ES and better clinical outcomes was not demonstrated in multivariate logistic regression analyses (OR, 0.530; 95% CI, 0.117 to 2.395; P=0.409). However, good outcomes after EVT were the absence of any post-procedural intracerebral hemorrhage (OR, 0.202; 95% CI, 0.054 to 0.759; P=0.018). Because ES had an interaction with post-procedural intracerebral hemorrhage (P=0.041), we speculate that ES has an indirect impact on worse clinical outcomes.
DISCUSSION
In the present study, we found that the prevalence of post-procedural ICH was relatively higher in patients who underwent emergent ES than in those who did not. Good outcomes after hyperacute extracranial artery treatment were attributable to multiple factors such as younger age, lower initial NIHSS score, successful reperfusion, and the absence of any ICH after EVT. Post-procedural ICH was related emergent extracranial artery stenting and associated with poor functional outcomes.
It is well known that EVTs such as mechanical thrombectomy are preferred to intravenous thrombolysis for intracranial large artery occlusions [9,17]. Whereas EVTs for intracranial large artery occlusions have had sufficient evidences of efficacy and safety, evidences for emergent ES have barely been achieved. Nevertheless, accumulating evidence has indicated the safety and efficacy of emergent endovascular stenting in hyperacute stroke. It was reported that endovascular therapy of tandem occlusions with extracranial internal carotid artery revascularization as the first step had a high recanalization rate and led to an acceptable rate of good clinical outcomes. However, little is known about the hemorrhagic risk after ES. A retrospective study about the hemorrhagic risk after emergent EVT with intracranial or ES showed that patients undergoing emergent stenting had higher grades of hemorrhagic subtypes, and acute phase stenting was an independent predictor of sICH after adjustment for potential confounders and the procedure duration. However, this study had a single-center retrospective design, and the sample size was small (24 patients) in the emergent stenting group [18]. Notably, TITAN study did not find a definite association between extracranial ICA stenting and post-procedural hemorrhage, although procedure-related complications after 90 days of EVT, including any ICH, were lower in the intracranial thrombectomy with ICA stenting group than in the intracranial thrombectomy only group [19]. However, while final successful reperfusion rate was similar between ES and NES groups in the current study, reperfusion success rate was significantly higher in the ICA stenting group than thrombectomy only group in the TITAN study. Reperfusion failure may increase the final infarct volume, which, in turn, can cause larger area of breakdown of blood-brain barrier and the risk of hemorrhagic transformation. Therefore, it is difficult to ascertain that ES-based EVT is safer than NES-based.
Several reasons may explain the relative high risk of ICH following ES in the current study. Many studies have suggested that hyperacute ICH after extracranial carotid artery stenting is mainly associated with abrupt cerebral hyperperfusion in the chronically hypoperfused areas [20-23]. The high rate of cerebral hyperperfusion after stenting is associated with the underlying diseases causing microangiopathy, high degrees of stenosis with the poor collateral flow, high degrees of stenosis on the contralateral carotid artery, and recent stroke history [20,21]. In addition, these post-procedural hemorrhages just after extracranial carotid artery stenting could result from rupture of small perforating arteries after rapidly normalized perfusion pressure in the chronically hypoperfused areas [24]. Prior usage of antiplatelets or anticoagulants might also increase the risk of post-procedural hemorrhage. In our current study, no significant correlation was observed between prior antiplatelet/anticoagulant medication and post-procedural hemorrhage. However, peri- or post-procedural antiplatelet treatment might potentially affect the incidence of ICH in the current study. As large infarct volume or microbleeds are seen on CT or magnetic resonance imaging, physicians may skip antiplatelet medication to escape hemorrhagic transformation. In contrast, physicians cannot skip the medication if ES is permanently deployed to escape in-stent thrombosis. Therefore, the occurrence of ICH after stenting might be caused by sudden hyperemia/hyperperfusion combined with post-stent prevention, such as antiplatelets.
Many studies have improved the process of EVT for intracranial large artery occlusion (LAO) in patients with acute ischemic stroke and tandem occlusion from ECAS disease. It is suggested that sufficient dilation of stenosis cervical artery is important for the successful use in stent-retrieval thrombectomy or spontaneous recanalization in cases of refractory LAO [25]. Therefore, it is necessary to perform balloon angioplasty or stenting for maintaining a good extracranial artery perfusion status. Our study showed that ES had an increased risk on post-procedure ICH; therefore, balloon angioplasty could be used as an alternative method, and cautious local administration of glycoprotein IIb/IIIa inhibitor, such as tirofiban, could be used to prevent re-occlusion of the extracranial artery after mechanical thrombectomy.
This study has several limitations. First, this study was a retrospective study; thus, the findings in the current study cannot be generalized. For escaping potential biases, we recruited multicenter data. Second, ICH after ES in patients with posterior circulation stroke was not well evaluated. Therefore, further studies must be implemented with a large amount of data related to extracranial vertebral artery stenting. Third, no exact data on pre- or post-stenting prevention were available; therefore, we could not exactly examine whether post-procedural ICH was related to stenting or/and antiplatelet medication during the stenting period. Therefore, further studies with a standardized dosage of antiplatelet medications before and after stenting are needed.
CONCLUSION
Emergent extracranial artery stenting has been used as a treatment option for hyperacute stroke patients with extracranial artery stenosis. This study found that ICH more frequently occurred in patients who underwent ES and was related to poor clinical outcomes in which ICH and ES had interaction. The findings indicate that ES must be cautiously considered in patients with ECAS-related acute ischemic stroke.