INTRODUCTION
Thrombectomy has become the standard of care for patients with large-vessel occlusions (LVOs) in the anterior circulation, leading to significant improvements in outcomes. However, a potential life-threatening complication associated with thrombectomy is hemorrhagic transformation (HT). In the realm of post-thrombectomy care, the recent integration of dual-energy computed tomography (DECT) allows for early differentiation between blood and iodinated contrast [1]. While there exists a consensus on the need for close monitoring and interventions when a hemorrhage is identified on immediate post-thrombectomy DECT [2], there is limited literature available on managing patients who do not exhibit immediate post-thrombectomy hemorrhage. Although relatively uncommon, some patients may undergo delayed HT, specifically delayed parenchymal hematoma (PH), which is associated with high morbidity and mortality [3,4]. Thus, it is crucial to identify patients who remain at high risk of developing delayed PH despite the absence of hemorrhage on immediate post-thrombectomy DECT.
Previously identified risk factors for PH at 24 hours following thrombectomy include age, smoking, elevated systolic blood pressure (SBP), congestive heart failure, thrombolytic administration, initial Alberta Stroke Program Early Computed Tomography Score (ASPECTS), and poor angiographic collateralization [3,5]. Recently, low levels of low-density lipoprotein cholesterol (LDL-C) have been suggested as a potential risk factor. While it is well-established that low LDL-C levels contribute to an increased risk of spontaneous HT in acute ischemic stroke (AIS) [6,7], emerging literature has proposed a possible association following intravenous and endovascular recanalization therapy [8,9]. For example, Lin et al. [8] suggested that LDL-C levels below 130 mg/dL could be a promising threshold for predicting HT after intravenous administration of thrombolytics. However, the literature on this topic is heterogeneous, with inconsistent results reported in other studies [10-13].
Given the conflicting data on the association between LDL-C levels and HT following the recanalization therapy for AIS and the lack of data in the setting of endovascular treatment, the aim of our study was to investigate the relationship between LDL-C levels and delayed PH following endovascular thrombectomy for anterior circulation LVO.
MATERIALS AND METHODS
Study Population
This study was approved by the Vanderbilt University Institutional Review Board (IRB #161778) and the requirement for informed consent was waived. Data were retrospectively collected for all patients who underwent thrombectomy for LVO at a comprehensive stroke center between January 2018 and December 2021. Among the initial cohort of 396 thrombectomy patients, 27 patients with posterior circulation LVO, 29 patients without immediate post-thrombectomy DECT or 24-hour imaging, and 141 patients with missing data were excluded. Furthermore, 17 and 23 patients were excluded due to the presence of subarachnoid and intraparenchymal hemorrhage, respectively, on immediate post-thrombectomy DECT. A total of 159 patients were included in the analysis.
Neuroimaging Protocol
Noncontrast computed tomography (NCCT), computed tomography angiography (CTA), and computed tomography perfusion (CTP) were performed before thrombectomy. The location of vessel occlusion was identified on the CTA. CTP provided the volumes of the infarct core (cerebral blood flow <30%) and penumbra (T-max >6 seconds). Recanalization after thrombectomy was evaluated by the thrombolysis in cerebral infarction (TICI) grading system [14]. TICI ≥2b, or filling of 51–99% of the ischemic territory, was considered successful recanalization [15].
All patients had DECT immediately post-thrombectomy and magnetic resonance imaging (MRI) or NCCT 24 hours afterward as routine standard of care. DECT was performed on a Siemens SOMATOM Force CT scanner (Siemens Healthcare GmbH). Virtual noncontrast images and iodine overlay map images with 5-mm slice thickness were generated using commercially available software with default parameter settings (syngo.via, DECT Brain Hemorrhage application version VB20A; Siemens Healthcare GmbH) to determine the presence of immediate post-thrombectomy hemorrhage. Delayed PH according to European Cooperative Acute Stroke Study III (ECASS III) criteria [16] was determined by 24-hour imaging (Fig. 1). All post-thrombectomy DECT, MRI, and/or NCCT were interpreted by a board-certified neuroradiologist.
Clinical Variables
Information on demographics, comorbid conditions, medication use, thrombolytic administration, presenting National Institutes of Health Stroke Scale (NIHSS), NCCT-based ASPECTS, CTP-derived infarct core and penumbra volumes, pre- and postprocedural SBP, time from last known well (LKW) to recanalization, location of vessel occlusion, stent retriever usage, number of thrombectomy passes, TICI score, and type of anesthesia was collected. The presence of hemorrhage on DECT and delayed PH on 24-hour imaging were recorded. Patients with hemorrhage on immediate post-thrombectomy DECT were excluded to select only those with delayed hemorrhage.
Outcome Measures
The primary outcome was the presence of delayed PH on MRI or CT performed 24 hours after endovascular thrombectomy.
Statistical Analyses
Data are presented as median and interquartile range (IQR) for continuous variables and as frequency for categorical variables. Pearson’s test or Fischer’s exact test was used to compare dichotomous variables between groups, while the independent sample 2-tailed t-test was used to compare continuous variables, as appropriate.
Univariable logistic regression analyses were employed to examine the predictive covariates for delayed post-thrombectomy hemorrhage (PH) observed on 24-hour imaging. Subsequently, a backward stepwise elimination process was conducted in R software to select relevant variables for inclusion in the multivariable logistic regression analysis. To account for potential confounders, covariate adjustment was performed using MATLAB software (MathWorks Inc.). The differential impact of LDL-C on delayed PH was investigated through covariate adjustments in MATLAB. The cut-off values of 50 and 100 mg/dL for LDL-C levels were determined based on the computation of OR for a range of LDL-C values (30, 40, 50, 60, 70, 80, 90, 100, 110, 120, 130, 140, and 150). The cut-off values were selected based on minimal P-values for the best discrimination process (Supplementary Table 1). Interaction analysis was performed using a 2-way analysis of variance test. Statistical significance was defined as a P-value below 0.05.
RESULTS
Description of Sample
A total of 159 patients without hemorrhage on post-thrombectomy DECT were included in the analysis. The median age of the cohort was 68 years (IQR, 19), and 48.43% were male. Delayed PH was observed in 18 patients (11.32%) on 24-hour imaging; 13 patients (8.18%) had PH type 1 (PH1), and 5 patients (3.14%) had PH type 2 (PH2). Of the 18 with PH, 12 patients were symptomatic. The baseline and clinical characteristics of the delayed PH and control groups are presented in Table 1. Patients with delayed PH had higher NIHSS (15 vs. 20; P=0.019), large CTP-derived penumbra volume (107 mL vs. 172 mL; P<0.001), lower high-density lipoprotein cholesterol (HDL-C) level (40 mg/dL vs. 37.5 mg/dL; P=0.044), lower LDL-C level (96 mg/dL vs. 76.5 mg/dL; P=0.040) than those without delayed PH.
Predictors of Post-Thrombectomy Delayed PH
In univariable analysis, delayed PH was associated with NIHSS (odds ratio [OR], 1.09; P=0.009; 95% confidence interval [CI], 1.02–1.16; per 1 score increase), CTP-derived penumbra volume (OR, 1.10; P=0.004; 95% CI, 1.03–1.18; per 10 mL increase), HDL-C (OR, 0.63, P=0.046; 95% CI, 0.40–1.00; per 10 mg/dL increase), and LDL-C (OR, 0.85; P=0.038; 95% CI, 0.72–0.99; per 10 mg/dL increase). In the multivariable model, LDL-C (OR, 0.76; P=0.038; 95% CI, 0.59–0.99; per 10 mg/dL increase) and CTP-derived penumbra volume (OR, 1.10; P=0.030; 95% CI, 1.01–1.20) independently predicted post-thrombectomy delayed PH (Table 2).
Differential Impact of LDL-C Levels on Post-Thrombectomy Delayed PH
In a subanalysis adjusted for potential confounders (age, anticoagulant or statin use, HDL-C, triglyceride, presenting NIHSS, CTP-derived infarct core and penumbra volumes, postoperative SBP, successful recanalization, number of thrombectomy passes, stent retriever usage), LDL-C ≤50 mg/dL (OR, 5.38; P=0.004; 95% CI, 1.70–17.04) was an independent predictor of post-thrombectomy delayed PH, while LDL-C >100 mg/dL (OR, 0.26; P=0.041; 95% CI, 0.07–0.96) was a protective factor (Table 3).
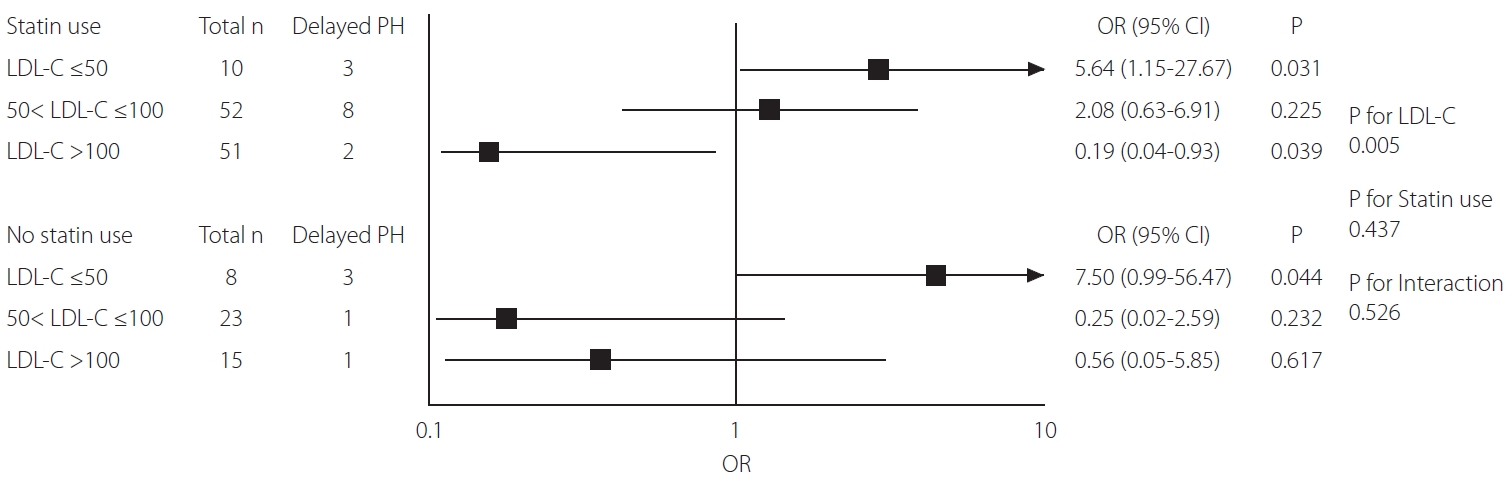
Furthermore, in a forest plot investigating the potential impact of LDL-C within subgroups of patients with and without prior statin use, LDL-C ≤50 mg/dL was associated with an increased risk of delayed PH regardless of statin use. In a subgroup of patients with prior statin use, LDL-C ≤50 mg/dL was significantly associated with an increased risk of delayed PH (OR, 5.64; P=0.31; 95% CI, 1.1–27.67), while LDL-C level >100 mg/dL were protective against delayed PH (OR, 0.19; P=0.039; 95% CI, 0.04–0.93). Among patients without prior statin use LDL-C ≤50 mg/dL was also significantly associated with a higher risk of delayed PH (OR, 7.50; P=0.044; 95% CI, 0.99–56.47) No significant interaction was found between LDL-C levels and statin use (Fig. 2).
DISCUSSION
In this study, lower LDL-C levels were associated with an increased risk of delayed PH at 24 hours following endovascular thrombectomy. Specifically, LDL-C ≤50 mg/dL independently predicted delayed PH, while LDL-C >100 mg/dL was a protective factor. Moreover, our study found no association between statin use nor other lipid levels, such as HDL-C and triglyceride, with post-thrombectomy HT. To the best of our knowledge, this is the first study that has examined the relationship between LDL-C and the risk of delayed PH specifically in the setting of endovascular recanalization of anterior circulation LVO.
The literature on the association between reduced LDL-C levels and HT following the recanalization of AIS remains heterogeneous. Previous studies have found that patients with HT following intravenous thrombolysis had lower levels of LDL-C than those without HT [8,9,17]. For instance, Lin et al. [8] suggested that LDL-C level ≤130 mg/dL can serve as a threshold to predict symptomatic HT within 24–36 hours after intravenous thrombolysis. However, some other studies found no significant association [10,11]. Furthermore, the data on the role of LDL-C in HT specifically in the setting of endovascular thrombectomy remains limited. Pikija et al. [18] investigated the contribution of serum lipid profiles to patient outcomes after endovascular thrombectomy for anterior circulation LVO. This study demonstrated that a high LDL-C concentration early in the course of anterior circulation LVO is independently associated with favorable clinical outcomes (modified Rankin scale ≤2) at 3 months. Similarly, Ha et al. [19] demonstrated that high LDL-C was associated with good functional outcomes at 90 days after thrombectomy. However, both studies did not assess the linkage between LDL-C and post-thrombectomy PH. Our findings suggest a possibility that the better functional outcomes among thrombectomy patients with high LDL-C may be attributable to the absence of delayed PH, although further investigation is needed.
The underlying biological mechanism of how LDL-C increases the risk of HT is not fully understood. It is suggested that lipids and cholesterols may play a role in maintaining the integrity of the arterial media layer of the smooth muscle as well as the endothelium of cerebral microvasculature [20]. Additionally, Zhou and Yang [21] proposed the double-hit hypothesis that exposure to low LDL-C levels induces functional and structural changes in endothelial cells and smooth muscle cells in the vessel walls, which subsequently make blood vessels more easily susceptible to bleeding in response to acute stressful environmental factors, such as AIS, intravenous thrombolysis, and/or neuroendovascular interventions. However, the biological mechanism of reduced levels of LDL-C increasing the risk of HT following endovascular thrombectomy is yet to be established and needs further investigation.
Moreover, our study did not find an association between HDL-C and triglyceride levels with HT following endovascular recanalization. A systematic review by Nardi et al. [22] demonstrated that there were no significant differences in HDL and triglyceride between AIS patients with and without HT. However, a recent systematic review and meta-analysis by Zhang et al. [23] found that HT after intravenous thrombolysis is associated with higher HDL concentrations. However, these studies included patients who only received intravenous thrombolysis, but no studies that investigated the association of HDL and triglyceride with HT in the setting of endovascular thrombectomy were found. Our study, which focused on endovascular thrombectomy, showed that HDL or triglyceride levels were not associated with HT following endovascular thrombectomy.
Statin use has been suggested as a possible risk factor for intracranial hemorrhage (ICH), especially among patients with prior history of AIS. For instance, the Stroke Prevention by Aggressive Reduction in Cholesterol Level (SPARCL) trial reported a small increase in the risk of ICH among AIS patients who are on intensive atorvastatin therapy [24]. However, subsequent studies have contradicted this finding. A population-based, propensity score-matched cohort study of 140,584 patients by Ribe et al. [25] showed that the risk of ICH was reduced in AIS patients who were statin users than those who were not. This is further supported by the retrospective cohort study of 8,535 patients by Scheitz et al. [26], which demonstrated no association between statin use prior to AIS and early HT, regardless of thrombolysis treatment. Additionally, this study showed that initiation of statin treatment after AIS was associated with reduced mortality. These findings are consistent with our finding that statin use is not associated with HT following endovascular thrombectomy, suggesting that the increased risk of HT in our cohort of thrombectomy patients may be due to low LDL-C levels as opposed to the direct side effect of the medication itself.
Lastly, our study revealed insignificant associations between the presenting NIHSS, NCCT-based ASPECTS, and CTP-derived infarct core volume with an increased risk of delayed PH following thrombectomy, which is in contrast with previous literature [3,27]. Nonetheless, our analysis identified a trend toward an increased risk of delayed PH in patients with higher presenting NIHSS, lower NCCT-based ASPECTS, and larger CTP-derived infarct core volumes, although statistical significance was not attained within our cohort. Moreover, our finding of insignificant association among thrombolytic administration, time to recanalization, and successful recanalization with delayed PH are in line with existing literature [28]. Nevertheless, it is important to note that the lack of significant associations in our study might be due to the limited sample size inherent in our single-center retrospective design. Consequently, further validation through large-scale, multi-center studies is warranted to ascertain the significance of these associations and enhance the generalizability of our findings.
There are several limitations that should be acknowledged. First, our study is a single-center retrospective study, which introduces the possibility of selection bias and confounding. Second, our study was conducted at a single comprehensive stroke center, which may limit the generalizability of our findings. Thus, multi-center prospective studies are needed to confirm our results in different and bigger populations. Third, although we adjusted for potential confounders in our analysis, there may be other unmeasured confounders that could influence HT following endovascular thrombectomy. For example, we did not include total cholesterol as a separate variable in our multivariable analysis. However, we believe a lower level of total cholesterol may be a surrogate marker for a low level of LDL-C, and thus we opted to divide total cholesterol into LDL-C and HDL-C for a more accurate assessment. Fourth, the thresholds to determine the differential impact of LDL-C on post-thrombectomy HT were determined subjectively. Future efforts should investigate varying cut-offs and thresholds to identify the optimal threshold for LDL-C that can reliably predict the risk of HT post-thrombectomy. Fifth, our analyses did not explore the potential association between LDL-C levels and immediate post-thrombectomy hemorrhages identified on DECT. Nevertheless, Ahn et al. [29] demonstrated that LDL-C is not predictive of either subarachnoid or intraparenchymal hemorrhage immediately post-thrombectomy. Existing literature has also suggested that immediate post-thrombectomy hemorrhages may be primarily attributable to mechanical factors associated with the procedure [30], or they may be linked to pre-existing infarcts prior to thrombectomy [31]. Therefore, we deemed it appropriate to exclude those individuals with immediate post-thrombectomy hemorrhages and focus solely on patients who experienced delayed PH occurring after the initial few hours. Lastly, it should be noted that the sensitivity and specificity of DECT may not be comparable to those of MRI. Consequently, there remains a possibility that certain patients with delayed PH might have experienced immediate post-thrombectomy hemorrhages that were undetected by DECT.
CONCLUSION
Our study suggests that low LDL-C levels (≤50 mg/dL) may be associated with an increased risk of delayed PH following endovascular recanalization of AIS, while high LDL-C levels (>100 mg/dL) may be protective. Additionally, no significant association was found among statin use, HDL-C, or triglyceride with HT after thrombectomy in this cohort. While the underlying mechanisms and causality of this association are not fully understood and require further investigation, patients presenting with LDL-C levels ≤50 mg/dL warrant close monitoring and necessary interventions, such as avoiding or reversing anticoagulation or lowering blood pressure, to prevent the development of delayed PH even in the absence of hemorrhage on immediate post-thrombectomy DECT.