INTRODUCTION
As diagnosis and management of stroke highly depends on the rapid assessment of large amount of information from imaging studies, automated methods using artificial intelligence (AI) may be applied at various stages in the evaluation and decision making [1]. Application of AI in stroke may range from the identification and triage of potential stroke patients to postprocessing of rapidly acquired images [2]. AI techniques have been applied in automatic or accurate diagnosis of stroke and its mechanism which may aid and expedite treatment initiation in an acute setting [3]. In addition, prediction of prognosis including development of hemorrhagic transformation and functional outcomes was achieved by various machine learning techniques [3]. There are ongoing research efforts for clinical application of AI techniques in stroke to accelerate and facilitate diagnosis and management of stroke and enable precision medicine.
Data curation is a prerequisite for developing AI models, and constructing a large database for various AI tasks in stroke requires a multicenter and multidisciplinary approach [4]. While imaging protocols for clinical trials are highly controlled and standardized, its application is impractical and unrealistic in routine clinical practice. On the other hand, a large amount of imaging data in stroke patients are acquired in routine clinical practice but imaging protocols and parameters remain highly variable. Previous nationwide survey of acute stroke imaging protocols for endovascular thrombectomy (EVT) reported considerable heterogeneity in acute stroke imaging protocols across South Korean tertiary hospitals reflecting hospital-specific conditions [5,6]. This supports the need to propose standardized and feasible imaging protocols for data curation in acute stroke.
In this study, we aimed to assess the current imaging protocols in acute stroke at tertiary hospitals in South Korea in the view of data curation and review evolving AI models to propose standardized and feasible imaging protocols.
METHODS
Survey
A nationwide, multicenter survey on acute stroke imaging protocols was conducted between April and May 2021 using an electronic questionnaire. A representative neurointerventionist or neuroradiologist at 43 registered tertiary hospitals certified by the Korean Society of Interventional Neuroradiology (KSIN) was contacted and the questionnaire was sent and collected electronically. The responses were analyzed using standard descriptive statistics (Microsoft Excel; Microsoft).
The survey consisted of multiple choice questions written in Korean with opportunities to provide additional comments if necessary. The first part was regarding the responderŌĆÖs hospital including the average number of patients with acute ischemic stroke treated with intravenous tissue plasminogen activator (IV t-PA) and EVT. The second part was subdivided into imaging protocols in the early time window, late time window and follow-up. The imaging protocols in the early time window was tailored for computed tomography (CT)- or magnetic resonance imaging (MRI)-based protocols. Imaging protocols for posterior circulation stroke were also evaluated.
Literature Review
A comprehensive literature search of publications on MEDLINE and EMBASE databases was conducted to identify original articles related to AI models in stroke imaging published up to November, 2022. The following search terms were used for screening ((ŌĆ£cerebral vascular diseaseŌĆØ) OR (ŌĆ£cerebrovascular diseaseŌĆØ) OR (ŌĆ£cerebrovascular accidentŌĆØ) OR (CVA) OR (stroke)) AND ((ŌĆ£artificial intelligenceŌĆØ) OR (ŌĆ£deep learningŌĆØ)) AND ((performance) OR (AUC) OR (sensitivity) OR (specificity)).
RESULTS
Survey
All 43 registered tertiary hospitals with a representative certified by KSIN participated in the survey, and included 18 (42%) regional emergency medical centers and 15 (35%) local emergency medical centers. There were 30 (70%) hospitals with 500ŌĆō1,000 inpatients, 6 (14%) with 1,000ŌĆō2,000 inpatients, 4 (9%) with 300ŌĆō500 inpatients, and 3 (7%) with more than 1,500 inpatients. Five to ten patients were treated with IV t-PA at 20 (47%) hospitals, and less than 5 patients at 15 (35%) hospitals per month. Less than 5 patients were treated with EVT at 22 (51%) hospitals, and 5ŌĆō10 patients at 17 (40%) hospitals per month. There were 25 (58%) hospitals with CT dedicated for emergency department and 13 (30%) with both CT and MRI dedicated for emergency department while 5 (12%) did not have dedicated CT or MRI for emergency department. Amongst hospitals performing MRI for acute ischemic stroke, only 3 Tesla (3T) MRI was used at 30 (73%) hospitals and both 3T and 1.5T MRI at 10 (23%) while only 1.5T MRI was used at 1 (2%) hospital.
Imaging protocols for IV t-PA candidates
For patients who presented within 4.5 hours of symptom onset and are considered candidates for IV t-PA, 15 (35%) hospitals performed noncontrast CT only, 14 (33%) performed noncontrast CT and CT angiography in a single session, and 13 (30%) performed noncontrast CT, CT angiography and CT perfusion in a single session.
Imaging protocols for EVT candidates in an early time window
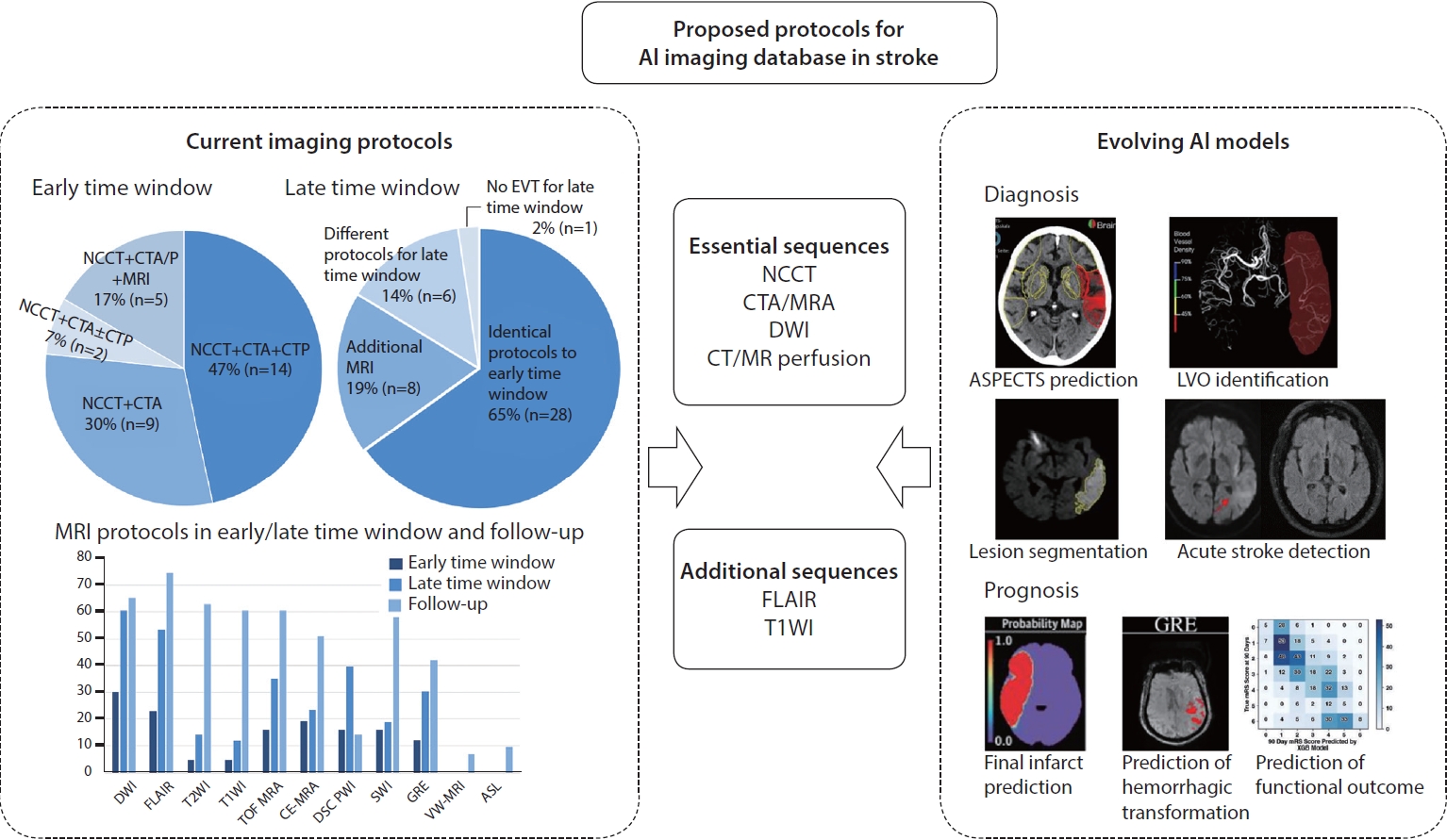
For patients who presented within 6 hours of symptom onset and are considered candidates for EVT, 30 (70%) hospitals performed CT-based protocols, 5 (12%) MRI-based protocols, and 8 (19%) combined CT and MRI protocols. The variation of CT- and MRI-based protocols and sequences adopted in MRI-based protocols are shown in Fig. 1.
Amongst 30 hospitals performing CT-based protocols, most hospitals (47%, 14/30) performed noncontrast CT, CT angiography and CT perfusion in a single session. Other hospitals performed noncontrast CT and CT angiography in a single session without CT perfusion (30%, 9/30) or performed CT perfusion selectively (7%, 2/30). For CT angiography, multiphase CT angiography (70%, 21/30) was more frequently performed than single phase CT angiography (30%, 9/30).
Amongst 13 hospitals performing MRI-based protocols or combined CT and MRI protocols, all hospitals (100%, 13/13) performed diffusion-weighted imaging (DWI) and 10 (77%) performed fluid-attenuated inversion recovery (FLAIR) image. There were 8 (62%) hospitals performing contrast-enhanced MR angiography (CE-MRA), 7 (54%) performing time of flight (TOF) MRA, and 7 (54%) performing dynamic susceptibility contrast (DSC) perfusion. There were 7 (54%) hospitals performed susceptibility-weighted imaging (SWI) and 5 (38%) performing gradient echo (GRE). There were 5 (38%) hospitals adopting fast MRI while 8 (62%) did not alter parameters to reduce scan time in an acute stroke setting.
Imaging protocols for EVT candidates in a late time window
For patients presenting after 6 hours and within 16 or 24 hours of symptom onset, 28 (65%) hospitals performed the identical protocol to that applied to patients presenting within 6 hours of symptom onset. The variation of CT- and MRI-based protocols and sequences adopted in MRI-based protocols are shown in Fig. 1. There were 8 (19%) hospitals performing additional MRI sequences for EVT candidates presenting in a late time window, which entailed converting from CT-based protocols in an early time window to combined CT and MRI protocols in a late time window in 7 (16%) hospitals. Different set of protocols was performed for EVT candidates presenting in a late time window at 6 (14%) hospitals, which entailed converting from CT-based protocols in an early time window to MRI-based protocols in a late time window. Noncontrast CT was performed at 34 (79%) hospitals, CT angiography at 28 (65%) hospitals, and CT perfusion at 16 (37%) hospitals. DWI was performed at 26 (60%) hospitals and FLAIR at 23 (53%). TOF MRA was performed at 15 (35%) hospitals, CE-MRA at 10 (23%), and DSC perfusion at 17 (40%). GRE was performed at 13 (30%) hospitals and SWI at 8 (19%). There were 10 (23%) hospitals using post-processing program for acute ischemic stroke that enabled estimation of infarct core and penumbra aiding treatment decision.
Imaging protocols in posterior circulation stroke
For acute ischemic stroke in posterior circulation, patients were considered for EVT if time from symptom onset to groin puncture was estimated to be within 24 hours at 19 (44%) hospitals, 12 hours at 7 (16%), and 6 hours at 2 (5%). There were no time criteria when considering candidates for EVT in posterior circulation at 15 (35%) hospitals. Identical imaging protocols to that used in anterior circulation stroke were used for posterior circulation stroke at 40 (93%) hospitals as it is difficult to differentiate posterior circulation stroke from anterior circulation stroke solely on the clinical grounds. Additional imaging was performed for posterior circulation stroke at 3 (7%) hospitals, which included performing DWI after CT-based protocol and additionally performing TOF MRA or CE-MRA.
Follow-up imaging protocols in acute ischemic stroke
Follow-up imaging studies within 1 week of acute ischemic stroke was performed in all patients at 27 (63%) hospitals. Patients underwent follow-up imaging studies only if treated with EVT at 13 (30%) hospitals and no follow-up imaging studies were performed at 3 (7%). Follow-up imaging studies were performed within 3 days of acute ischemic stroke at 26 (60%) hospitals, within 5 days at 7 (16%), and within 7 days at 6 (14%).
For follow-up imaging, CT and/or MRI-based protocols were adopted. Noncontrast CT was included at 13 (30%) hospitals and CT angiography at 5 (12%). No hospitals included CT perfusion during follow-up. For MRI-based protocols, FLAIR was included at 32 (74%) hospitals, and DWI at 28 (65%). T2-weighted imaging (T2WI) was included at 27 (63%), T1-weighted imaging (T1WI) at 26 (60%), CE-T1WI at 15 (35%). SWI was included at 25 (58%) hospitals, and GRE at 18 (42%). TOF MRA was included at 26 (60%) hospitals, CE-MRA at 22 (51%), DSC perfusion at 6 (14%) and arterial spin labelling at 4 (9%). Vessel wall imaging was included at 3 hospitals (7%).
Literature Review
Main applications of AI in stroke include supporting detection of key imaging characteristics and predicting outcomes. During acute phase, AI can support detecting acute ischemic lesion including infarct core or potentially salvageable tissue, large vessel occlusion or hemorrhage. AI can also be used to predict short-term imaging outcome such as final infarct or hemorrhagic transformation and long-term functional outcome. The required imaging sequences used to develop AI models in acute stroke are summarized in Table 1. Of 26 studies, 18 (69%) studies were conducted at a single center while 8 (31%) were multicenter studies. The sample size ranged from 34 patients in a single center setting to 1,383 patients in a multicenter registry [7,8]. The AI algorithms were assessed using performance metrics such as sensitivity, specificity, accuracy, area under the receiver operating characteristic curve, F1 score, correlation and dice indices.
AI models have been developed to support diagnosis in an acute setting or estimate stroke volume in subacute or chronic stage. For determination of Alberta Stroke Program Early CT Score (ASPECTS), follow-up CT or DWI were used to establish ground truth and predict ASPECTS on the baseline CT [7,9,10]. The model using DWI as the ground truth showed higher specificity than the models using noncontrast CT alone (94.2% vs. 57.0%). In addition, one of the CT-based models used DWI as the ground truth while MR-based models were based solely on MR images. For identification of stroke within 4.5 hours, MRI sequences such as DWI and FLAIR as well as parameters such as Tmax from DSC perfusion were used to detect acute ischemic lesions [11,12]. The inclusion of DSC led to an improvement in sensitivity (89.3% vs. 72.7ŌĆō75.8%). For identification of large vessel occlusion, multimodal CTs including noncontrast CT, CT angiography and CT perfusion were used to determine large vessel occlusion on CT angiography [13,14]. The model performance in identification of large vessel occlusion was comparable with or without CT perfusion. For automatic lesion segmentation, DWI was used to detect infarct core and noncontrast CT to detect hemorrhagic stroke [15-17]. For automatic lesion segmentation in the subacute and chronic stage, FLAIR and T1WI were used respectively [18,19].
AI models have also been developed to predict final infarct, hemorrhagic transformation and functional outcome. For predicting final infarct, there were a small number of studies using noncontrast CT, CT angiography or CT perfusion although most studies were MR-based using information on DWI, FLAIR and DSC perfusion to predict final infarct defined on FLAIR or DWI with AUC of up to 0.92 and accuracy of up to 84% [20-24]. AI models using CT as the input data offered quantitative outcome measures such as correlation of the final infarct volume but did not provide anatomical outcome measures such as overlapping ratio between ground truth and predicted region of interest masks as in AI models using MRI. For hemorrhagic transformation, ground truth was defined on follow-up GRE or noncontrast CT, and information on noncontrast CT as well as MRI sequences such as DSC perfusion and DWI were used [25-27]. For predicting functional outcome such as successful recanalization following EVT and functional scores such as modified Rankin scale or national institute of health stroke scale, noncontrast CT as well as CT angiography and CT perfusion were used along with multiple clinical and laboratory parameters [8,28,29]. For predicting outcome such as visual field, motor function and cognition, three-dimensional T1WI was commonly used as well as T2WI, FLAIR and DWI for lesion segmentation [30,31]. MRI-based prediction of functional outcome with inclusion of T1WI resulted in prediction accuracy of up to 91.3% [30]. Information on functional MRI enabled correlating lesion topography and network dysfunction in accounting for behavioral deficit.
DISCUSSION
Our study aimed to assess the current imaging protocols in acute stroke at tertiary hospitals in South Korea and review required imaging sequences for developing AI models in stroke. A nationwide survey involving 43 registered tertiary hospitals revealed considerable heterogeneity in the imaging protocols for EVT candidates in the early time window, late time window and posterior circulation stroke. In addition, indication and imaging protocols for follow-up MR imaging differed considerably. Required imaging sequences for developing AI models for diagnostic and prognostic purposes were reviewed. The commonly used sequences were noncontrast CT, CT angiography and DWI for diagnostic purposes while FLAIR, DSC perfusion, and T1WI were additionally required for prognostic AI models.
Heterogeneity in Imaging Protocols in Acute Stroke Imaging
The result of our survey was consistent with the findings of previous nationwide surveys which reported considerable heterogeneity in acute stroke imaging protocols [5,6]. The imaging protocol is inherently influenced by the medical resources and hospital-specific circumstances as reflected by variable availability of emergency department dedicated CT (84%) and MRI (12%) revealed by the current survey. CT-based protocols were preferred (70%, 30/43) for EVT candidates in an early time window while more hospitals adopted MRI-based or combined CT and MRI protocols in a late time window. For EVT candidates in an early time window, noncontrast CT and CT angiography were performed in all patients undergoing CT-based protocols. For EVT candidates in a late time window, more hospitals performed MRI-based protocols or additional MRI sequences as shown by previous nationwide surveys [5,6].
For MRI-based or combined CT and MRI protocols, DWI was most frequently performed MRI sequence in both early (30%, 13/43) and late time windows (60%, 26/43) as well as posterior circulation stroke (70%, 30/43). FLAIR was the second most frequently performed MRI sequence for EVT candidates in both early (23%, 10/43) and late time windows (53%, 23/43) while there were more variations in performing other MRI sequences such as MRA, MR perfusion, T2WI, T1WI, GRE, and SWI. During follow-up, FLAIR was the most frequently performed MRI sequence (74%, 32/43) and there was a particularly frequent inclusion of T2WI (63%, 27/43) and T1WI (60%, 26/43). Additional MRI sequences such as arterial spin labelling and vessel wall MRI were also performed only during follow-up.
Required Imaging Sequences for AI Model Development in Acute Stroke
In an acute stroke setting, detecting imaging findings that indicate acute ischemia and large vessel occlusion are critical in screening appropriate candidates for EVT. For AI models for detecting acute ischemic lesions, noncontrast CT and DWI were most commonly used as input images as well as reference standard. For identification of large vessel occlusion, CT angiography was most commonly used. For identifying stroke within 4.5 hours, FLAIR and DSC perfusion were additionally used.
For prognostic purposes, noncontrast CT was used for predicting hemorrhagic transformation. CT angiography and CT perfusion were used to predict treatment and functional outcome. DWI, FLAIR and DSC perfusion were used to predict final outcome with FLAIR used as a reference for the final infarct. Three-dimensional T1WI was used for co-registration purpose in predicting for delicate functional outcomes.
Proposed Protocols for AI Imaging Database in Stroke Imaging
It is important to propose feasible and standardized protocols in order to construct imaging database for AI in acute stroke. We hereby propose such protocol taking into account of the considerable heterogeneity in the current acute stroke imaging protocols and required imaging sequences for AI model development (Fig. 1).
Noncontrast CT should be included as a baseline study as it was performed for all IV t-PA candidates and most commonly used as input images and reference standard for important AI tasks such as determining ASPECTS, identifying large vessel occlusion, and predicting hemorrhagic transformation. CT angiography, which was always performed along with noncontrast CT for EVT candidates in an early time window, should also be included if CT-based protocol is adopted as CT angiography may be used in identifying large vessel occlusion and predicting functional outcome. As shown by this nationwide survey, multiphase CT angiography may be preferred over single phase CT angiography.
Despite the universal use of noncontrast CT in stroke imaging, however, the inherent limitation in detecting and segmenting acute ischemic lesions and hemorrhagic transformation solely on noncontrast CT is well-recognized [32] accounting for currently lower AI algorithm performance than MRI-based algorithms [20,21]. DWI, which was the most frequently performed MRI sequence in the early and late time windows and posterior circulation stroke, formed the basis for developing most AI models in identifying stroke within 4.5 hours, automatic lesion segmentation, and predicting final infarct by serving as the ground truth as well as input images. FLAIR, as second most frequently performed MRI sequence, should also be considered as it is used to identify of stroke within 4.5 hours and predict final infarct and functional outcome. Perfusion imaging including DSC perfusion or CT perfusion should also be considered for predicting final infarct and prognosis as identification of penumbra size plays a vital role in treatment decision for mechanical thrombectomy. Moreover, it is important to obtain baseline and posttreatment angiography for evaluating treatment outcome of EVT, and recanalization is an important factor for prognosis as well as hemorrhagic transformation [33].
Despite the lack of universal inclusion of T1WI in the early and late time windows, T1WI may serve an important role in the co-registration process for developing AI models. The survey showed that T1WI was performed at 60% of hospitals during follow-up of acute ischemic stroke. While T1WI obtained during follow-up may be used for co-registration purpose, lack of corresponding T1WI in the early and late time windows may limit the scope of tasks for AI models, and the possibility of using DWI and FLAIR for co-registration purpose is being increasingly explored.
Combined CT and MRI based protocols consisting of noncontrast CT, DWI, FLAIR, DSC perfusion, T1WI, and CT/ MR angiography are likely to offer strong foundation for constructing AI imaging database in acute stroke. With attempts to accelerate MRI acquisition [34], more MRI sequences may be incorporated due to inherently limited amount of information available on noncontrast CT. Given the considerable heterogeneity in the imaging protocols amongst hospitals at each time window, it is impractical to propose an identical imaging protocol in acute stroke. As seen in recent largescale clinical trials, more efforts should be directed in unifying baseline and posttreatment protocols in order to allow intra-individual comparison while ensuring quality control of the obtained images. Moreover, standardization of treatment outcome using clinically validated measures such as arterial occlusive lesion scale or modified treatment in cerebral ischemic scale should be emphasized [33]. In addition, clinical information such as accurate last known normal times should be collected together.
Limitations
There were several limitations in this study. While this nationwide survey with 43 participating hospitals successfully demonstrated considerable heterogeneity in imaging protocols in acute stroke, only the hospitals with members certified by KSIN were invited to participate in the survey. Given that the South Korean government designated 150 hospitals as local or regional emergency medical centers, the current status at 43 tertiary hospitals may not reflect the true real-world variation. In addition, the survey did not consider clinical outcome of the imaging protocols and the proposed protocols were based on the feasibility and standardization of the protocols rather than clinical impact. Although many AI models developed in stroke were reviewed, extensive search of literature with systematic meta-analyses may provide more comprehensive compilation of required imaging sequences. The model performance of AI models was presented with variable parameters resulting in limited comparison of model performance developed with different combination of imaging modalities and sequences.
CONCLUSION
In conclusion, AI heavily relies on data curation and there is a need to propose standardized and feasible imaging protocols given the current considerable heterogeneity in acute stroke imaging protocols. The essential sequences may be noncontrast CT, DWI, CT/MR angiography, and CT/MR perfusion while FLAIR and T1WI may be additional used for prognostic AI models. MR-based AI models currently offers detailed anatomical outcomes with superior performances while further research is required to improve the performance of AI models based on CT protocols. Moreover, identical imaging protocols from baseline to follow-up evaluation are recommended.