Large and giant carotid cavernous aneurysms (CCAs) tend to cause mass effect, manifesting ocular motor nerve palsy and trigeminal neuralgia. They have been treated with simple coil packing with balloon or stent assist techniques for such symptomatic aneurysms. However, these methods are not always effective against the decompression of cranial nerves because of the f illed coil mass in the sac, and the symptoms occasionally worsen due to regrowth of the aneurysm. Parent artery occlusion has been thought of as the most effective way to achieve recovery from cranial nerve palsy due to large CCAs [1]. It can stop all inflow to the aneurysm in exchange for the loss of one carotid artery. However, in cases of poor collaterals, extra-intracranial arterial bypass surgery should be required.
Flow diversion (FD) has been introduced as an alternative option for treating large cerebral aneurysms. FD can promote aneurysm occlusion through a process of endoluminal reconstruction of the parent artery and by rectifying blood flow away from the aneurysm sac [2]. Specifically, positive results of a PipelineŌäó embolization device (PED) (Medtronic/Covidien, Irvine, CA, USA) have been demonstrated in several recent series [2,3,4,5]. In the present study, we review our case series of patients treated with PED, and discuss the efficacy and safety of the flow diverter by comparison with other conventional treatment options.
MATERIALS AND METHODS
Patient and aneurysm profile
An endovascular approach was used to treat 59 patients with unruptured large and giant CCAs between December 2012 and December 2016 at Nagoya University and Osaka Medical College. After obtaining institutional review board approval from each institution, we searched our prospectively maintained database for all patients with unruptured CCAs. Twenty four aneurysms in 24 patients (23 women and 1 man; 40-86 years old; mean age 71.5 years) were treated with PED. We retrospectively reviewed the patients' medical charts to determine the patient prof iles, aneurysm characteristics, procedural specifics, and procedural complications. Only clinically relevant procedural complications are reported here. Radiological studies, including angiography, MRI, and CT were carefully reviewed pre- and postoperatively and at 6 months follow-up.
Of the 24 aneurysms, 16 were located on the right side, and the mean max. dia. was 19.4 mm. There were 18 large aneurysms and six giant aneurysms. Fourteen patients had a single aneurysm, and six patients had another aneurysm in addition to a CCA. Eighteen patients suffered ocular motor palsy, and 1 patient suffered ocular pain. Six patients were asymptomatic.
All 24 patients were pre-medicated with anti-platelet agents for 7 days before the intervention. The patients were pre-loaded with 75 mg of clopidogrel and 100 mg of aspirin daily. Treatment was performed with an initial 5,000 IU heparin bolus and the intraoperative maintenance of an activated clotting time of two times of the patient's baseline value. Anti-platelet function was checked preoperatively with VerifyNow┬« (Medicos-Hirata, Osaka) for all patients, and further anti-platelet agents were loaded for hypo-responders (PRU>250). Heparin was discontinued at the conclusion of the procedure. Dual antiplatelet therapy was continued for Ōēź6 months after the procedure.
Deployment of PED
With the patient under general anesthesia, a 6 Fr. super-long sheath (ShuttleŌäó sheath, Cook Medical, Bloomington, IN) and a coaxial 5 Fr. or 6 Fr. distal access catheter (NavienŌäó, Medtronic/Covidien) were placed in the ICA, and a microcatheter (MarksmanŌäó, Medtronic/Covidien) for stent delivery was placed distal to the aneurysm. A PED was carefully deployed using the unsheath or ŌĆ£center & pushŌĆØ method [6]. After the stent was deployed, vessel wall apposition was remedied with a micro-balloon (Hyperform; Medtronic/Covidien) angioplasty in all cases, and the state of expansion of the PED was confirmed on conebeam CT. The f inal angiogram was checked to determine the reduction of the inflow to the aneurysmal sac (expressed as an eclipse sign) and intra-stent rectification of the carotid flow. We used a single stent in all cases except for one case that required telescoping overlapped stents because of the insufficient effect of the flow diverter on the single stent. No coils were placed in the aneurysmal sac.
Clinical and radiological follow-up
The primary clinical outcome was the status of cranial nerve deficits produced by the mass effect. The final clinical status was assessed at the 6-month follow-up. The registered complications were ischemic events, hemorrhagic stroke, aneurysm rupture and increased mass effect. We collected clinical outcomes at the last available follow-up from follow-up notes of the attending physician and classified them using the modified Rankin Scale.
We classif ied the occlusion state just after the treatment into three categories according to the Roy and Raymond scale [7]: complete occlusion (CO) including no visualization of the aneurysmal sac as well as the parent artery occlusion; neck remnant (NR); and body filling (BF) with the remnant sac. Although no immediate occlusion of the aneurysmal sac was found in most patients, the rectifying effects were recognized as a blurred or partial opacification of the aneurysm due to the subtraction of remaining stagnated contrast in the sac expressed as an ŌĆ£eclipse signŌĆØ.
A radiological follow-up for each patient (digital subtraction angiography [DSA] or magnetic resonance angiography [MRA]) was scheduled for 3-6 months after treatment. Any aneurysms observed at the 6-month follow-up were classified with the same scale again, and aneurysms that displayed a decreasing percentage of occlusion (>10%) on follow-up angiography were considered recurrent.
RESULTS
The patient summary is shown in Table 1, and profiles and results are shown in Table 2. There was only one case of immediate aneurysm obliteration, and all of the other aneurysms were filled to some degree (regarded as body f illing) and showed the typical eclipse sign, except for two cases.
At the 6-month follow-up, 16 of the 24 aneurysms were found to be completely obliterated, and among the five remaining aneurysms a small leak from the PED was observed at the neck in four, and major body filling remained in one (Case 13). On MRI, follow-up some degrees of size reduction were observed in all aneurysms.
Among the 18 symptomatic patients with ocular motor nerve def icits or visual disturbances, an improvement of symptoms before 6 postoperative months was obtained in 16 patients, including cures in 6 patients.
Newly developed or worsened ocular motor nerve palsy was temporarily observed in 7 patients. Oculomotor palsy was observed in addition to abducens palsy in five patients, ocular motor nerve palsy was newly developed in three patients, and worsening of existing abducens palsy was found in two patients. The timing of the manifestations of these symptoms occurred at an approximately 3-week interval, and all of them disappeared or improved within 3 months.
There was one procedure-related complication with ischemic events; a case of telescoping stent due to the complicated procedure (Case 2). Temporary hemiparesis and aphasia completely resolved at one month. We encountered two asymptomatic hemorrhagic complications, probably due to the hyper-response of antiplatelet agents.
Representative cases
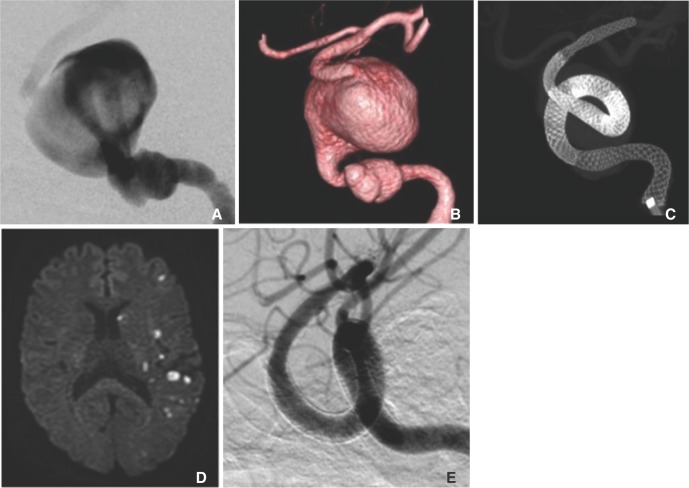
Case 1: A giant aneurysm of complete occlusion(Case No. 1)
This 40-year-old male was suffering from progressive right abducens palsy. He had a giant CCA protruding laterally at the right side (Fig. 1A). A PED (4.0├Ś25 mm) was successfully deployed with a marked eclipsed sign (Fig. 1C). His symptoms were resolved at the 3-month follow-up, and the angiogram taken at 6 months showed complete occlusion of the aneurysm (Fig. 1D). The aneurysm was found to have shrunk in the MRI (Fig. 1E, F).
Case 2: A giant aneurysm requiring a telescoping stent (Case No. 2)
A 48-year-old female had suffered from progressive double vision and headache for 4 years. She presented with total abducens nerve palsy on the left side. Left carotid angiogram disclosed a no-necked giant CCA and another tandem aneurysm on the near proximal side (Fig. 2A, B). Five PEDs were connected with partial overlapping to cover the neck of both aneurysms in two stages (Fig. 2C). The final angiogram showed a significant flow diversion effect with a typical eclipse sign. However, she suffered from right hemiparesis and mild aphasia for 1 month because of the long, complicated procedures. Post-MRI showed multiple small ischemic lesions due to the showered thromboemboli (Fig. 2D). Her symptoms remained at 6 months, but the aneurysm was completely resolved on the angiogram (Fig. 2E)
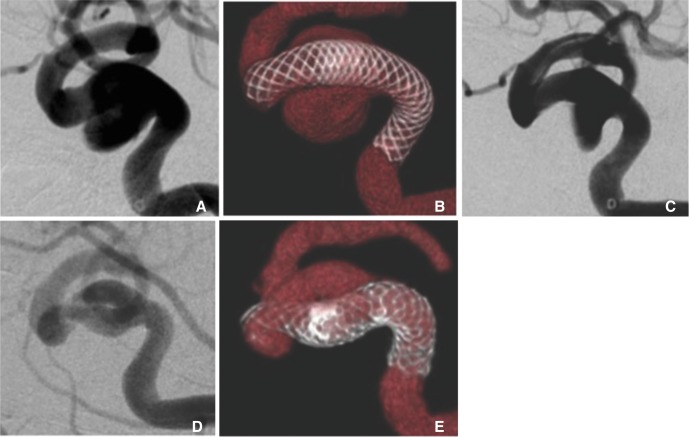
Case 3: A case of remaining neck on the follow-up(Case No. 11)
This 80-year-old female complained of double vision due to complete abducens and mild oculomotor palsy beginning 6 months ago. She had a large CCA at the right side (Fig. 3A) and underwent a PED (4.0├Ś25 mm) deployment (Fig. 3B). The angiogram obtained just after the treatment demonstrated a typical eclipse sign, suggesting stagnating intra-aneurysmal flow (Fig. 3C). Two weeks later, her ocular symptoms had worsened to complete oculomotor palsy with severe ocular pain. Her symptoms gradually improved due to steroid medication and completely subsided 3 months later. A follow-up angiogram at 6 months showed that the PED had sunk into the aneurysmal sac due to the loss of an anchoring effect associated with shortening of the distal side, and the original pathway was left with a remnant neck (Fig. 3D, E).
DISCUSSION
A flow diverter is a key device for large and giant cerebral aneurysms. The Pipeline embolic device (PED) is the only flow diverter device approved in Japan. PED, which closes the orif ice with a dense woven mesh and, while conserving the parent artery, promotes natural internal thrombolization, is a device developed based on a completely different concept compared to coil embolization [3,4].
The efficacy of flow diverters has been demonstrated in previous studies. Puffer et al. [7] reported that 36% of the patients in their series showed procedure-related or delayed complications but no clinical sequelae [8]. The mortality rate associated with flow diverter use was 0%-4% in many studies [2,3,4,5,8,9,10,11,12,13]. The rate of occlusion of an aneurysm with a flow-diverting stent is higher than that of the usual coiling method with adjunctive techniques [12,13]. A multicenter study showed 71-86% complete occlusion rates, and no recurrence [14,15]. Ocular motor palsy symptoms were relieved within 3 months in more than 90% of symptomatic patients in our series. However, seven of 18 symptomatic patients showed temporary deterioration of ocular motor nerve palsy. This strange course may be due to the strong inflammatory reaction of the aneurysmal wall along the progressive thrombosis in the aneurysmal sac. Thrombosis leads to a strong mural inflammation of the blood vessel. Such a vital reaction is commonly found at the connective tissue around thrombosed veins as well as in embolized experimental aneurysms [16]. Inflammation that extends around the aneurysmal sac can affect the neighboring cranial nerves, resulting in the deterioration or loss of their function. This mechanism is supported by MRI findings of luminal enhancement of the aneurysm wall and the dramatic effects of steroid administration [17].
In our series, this deterioration was encountered approximately two weeks after the deployment of PED. According to our cohort study comparing another treatment option, stent-assisted saccular coil packing [6], such manifestations tended to be more delayed in PED cases than in cases with coil embolization. We posit that this time lag is related to the differences in timing of thrombosis formation. Intra-aneurysmal thrombosis is achieved just after the saccular packing, while it should take some interval to complete the whole thrombosis after the intra-aneurysmal flow stagnation due to the flow diverting effect.
The safety of treatment with PED has recently increased [11,19]. In particular, an advanced version of PED, the Flex type, has improved quality and maneuverability thanks to the structural changes, which simplifies and facilitates initial deployment. The pusher wire has been replaced by a larger, elongated hypo-tube to permit better pushability. The Flex type is almost completely re-sheathable due to the introduction of a re-sheath pad [20]. However, the temporary procedure-related adverse events have not yet been diminished [21]. Previous reports show 4.7 to 6.6% of patients develop ischemic complications, particularly patients who hypo-respond to anti-platelet agents, and incomplete apposition of PED [14,15]. We preoperatively checked the effect of anti-platelet therapy for all patients and forced anti-platelet management with additional agents if the result showed insufficient values. Further, we usually added balloon angioplasty to attach the strut to the vessel wall using a balloon catheter (7├Ś7 mm) (HyperformŌäó, Medtronic/Covidien) in all cases [6]. That is why we did not encounter thrombotic occlusion of the parent artery and branches. However, shortening of PED with deviation into the aneurysmal sac was observed in two cases at follow-up imaging (Case 11, 17), resulting in the remnant neck. These conditions are now carefully observed, and for the case of persistent incomplete occlusion, overlapped FD should be considered. As an inevitable diff iculty of a bladed-type stent, an unexpected shortening or elongation can occur depending on the diameter of parent artery. It is important to evaluate and estimate the expected length corresponding to the proper initial and landing position [21].
The use of a flow diverter was more beneficial than the conventional techniques in terms of safety, efficacy and cost compared to the conventional parent artery occlusion and saccular coil packing techniques [9,18]. Flow diverters completely seal the aneurysm neck with their diverting effect and lead to aneurysmal thrombosis and shrinkage and support the diseased vessel, allowing its remodeling [22]. The re-establishment of homeostasis may contribute to a favorable angiographic and physical state, and the amelioration of symptoms. Although longer follow-up data are essential to precisely determine the efficacy, from a cost-effective and time-saving viewpoint, PED is a relatively safe and reliable method for the treatment of large CCAs.